Download
1 / 38
380 likes | 596 Vues
China and South Africa. Ellie Ingram, Chami Pang, Allie Cabral, Erica Falls, Jenny Thay. China’s Geography. Total area: 9,596,961 sq. km. (about 3.7 million sq. mi.). Capital --Beijing. Terrain: Plains, deltas, and hills in east; mountains, high plateaus, deserts in west.

E N D
China and South Africa Ellie Ingram, Chami Pang, Allie Cabral, Erica Falls, Jenny Thay
China’s Geography • Total area: 9,596,961 sq. km. (about 3.7 million sq. mi.). • Capital--Beijing. • Terrain: Plains, deltas, and hills in east; mountains, high plateaus, deserts in west. • Climate: Tropical in south to subarctic in north.
Demographics • Population: 1,336,718,015 • Life expectancy: 74.68 years • Infant Mortality Rate: 16.06 deaths/1,000 live births • Death Rate: 7.03 deaths/1,000 population • Literacy Rate: 92.2%
Socioeconomic Conditions • Second largest producer in GDP • They became the preferred destination of relocations of global manufacturing facilities, the second largest importer of crude oil and the fifth largest producer of energy • 5 year plans to improve the economy by lowering inflation, improving social infrastructure and increase consumption • Population and Family Planning Law which only allows one child per family, hoping to stabilize their large population which they believe will grow over 1.4 billion by the year 2026.
Government System • Communist Led country but not dictatorship • Divided into 3 main parts: • National People’s Congress, the President and the State Council • National People’s Congress is the highest ranking power which is elected through democratic vote
Its duty includes the power amend and enforce the constitution, elect president and make decisions affecting peace and war. NPC elects the President and supervises the State Council President is China’s head of state. In charge of some decision making, appointing such as premier and State Council but doesn’t have administrative power for he must do everything under the NPC State Council acts by virtue of authority of NPC, formulate administrative orders and duties such as monitoring implementation and prepare economic plan. There are two sections of organizations in the government, the Ministerial which runs activities such as Ministry of Commerce and Geographical that takes cares of include provincial, local and municipal government China’s government system consists of tier rankings and every ranking must report to those above it unlike the US’s government system which power is balanced out by levels of government.
Performance • Indicators of the status of China’s health sector can be found in the nation’s fertility rate of 1.8 children per woman (a 2005 estimate) and the infant mortality rate per 1,000 live births was 25.3 (a 2004 estimate) . • In 2005 China had about 1,938,000 physicians (1.5 per 1,000 persons) and about 3,074,000 hospital beds (2.4 per 1,000 persons). Health expenditures were US$224 per capita in 2001, or 5.5 percent of gross domestic product (GDP) . Some 37.2 percent of public expenditures were devoted to health care in China in 2001. However, about 80 percent of the health and medical care services are concentrated in cities, leaving timely medical care is not available to more than 100 million people in rural areas. • Healthcare expenditures as a percentage of GDP have been increasing in China over the past 20 years, but remain low when compared to developed countries. • China spent 5.8 percent of its GDP on healthcare in 2002.
Healthcare Expenditures by source of Payment • As shown, the percentage of out-of-pocket health expenditures have increased since the 1990’s. • In 2003, almost 45 percent of the urban population and 79 percent of the rural population had to pay for medical services out-of-pocket. • 3 formal infrastructures of healthcare funding: • Government • Labor Health Insurance/ Urban Employee Basic Medical Insurance System (UBEMIS) • (RCMS); rural cooperative medical system
Healthcare funding: Government Government Employee Health Insurance provides coverage for government workers at all political divisional levels), including officials of labor unions, youth's and women's leagues, the staff of cultural, educational, health and research institutes and students at approved colleges and universities. in 1992, 30 million people were covered by the government system. Health services are mainly provided by public hospitals, but larger organizations with more than 200 employees usually set up their own clinics. The beneficiaries of the Chinese government are required to seek health services at appointed hospitals of the organization, and the charge for the services is reimbursed by the governmentbased on the government fee schedule. The Chinese government is responsible to fund public health services provided by public, non-profit service providers, such as health centers and smaller hospitals. This includes the controlling and preventing infectious diseases, administering immunizations and treating mental illness. a “basic” medical services package that is intended to be affordable and available for all citizens. It should, at a minimum, cover prenatal care, routine check-ups, emergency services and treatment of common diseases, such as diabetes.
Healthcare funding: UEBMIS • The second form of funding provided to some citizens is Labor Health Insurance , a system under which employees in state and collective enterprises and their immediate family members are entitled to full (for the employees themselves) or partial (for immediate family members) benefits. Government rules that the state enterprises with more than 100 employees must provide labor health insurance. Payment is made mainly out of "welfare funds" of enterprises, a portion of which are for medical services.
Healthcare funding: RCMS The New Rural Co-operative Medical Care System (NRCMCS) is a 2005 initiative to overhaul the healthcare system, particularly intended to make it more affordable for the rural poor . Under the NRCMCS, the annual cost of medical coverage is 50 yuan (US$7) per person . Of that, 20 yuan is paid in by the central government, 20 yuan by the provincial government and a contribution of 10 yuan is made by the patient . As of September 2007, around 80% of the rural population of China had signed up (about 685 million people) . The system is tiered, depending on the location . If patients go to a small hospital or clinic in their local town, the system will cover roughly 70-80% of their bill . If the patient visits a county clinic, the percentage of the cost being covered falls to about 60% . If the patient requires a specialist in a modern city hospital, the plan would cover about 30% of the bill.
Workforce • There have been significant improvements in raising the quality of healthcare personnel. However, quality has to be further enhanced to increase the level of patient care. There is no uniform definition to document the required qualifications of healthcare personnel . Current training and experience of healthcare personnel is relatively weak. According to Brian Wong, in a 2001 study of 46 counties and 781 village doctors in 9 Western provinces found that 70 percent of village doctors had no more than a high school education, and had received an average of only 20 months of medical training. Not only are there fewer personnel in rural areas, it is very difficult to attract and retain skilled personnel to work in less developed regions of China.
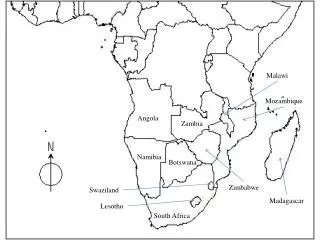
Introduction • Size & Geography: - Total area: 1, 219, 090 sq. km - 9 official provinces; • The Eastern State • The Free State • Gauteng • KwaZulu-natal • Limpopo • Mpumalanga • The Northern Cape • North west • The Western Cape - Bordered by the Atlantic Ocean on the western side and the Indian Ocean on its eastern side.
Demographics • Total population (July 2011): 49,004,031 - Ethnic groups: • Black African 79% • White 9.6% • Colored (Indian/Asian) 11.4% -Age groups: ( “estimates for this country take into account the effects of excess mortality due to AIDS” ) • age 0-14 (28.5%) • age 15-64 (65.8%) • age 65+ (5.7%) -Birth rate: 19.48 births/1,000 population -Death rate: 17.09 deaths/1,000 population -People living with HIV/AIDS (2009): 17.8% (5.6 million) -Deaths from HIV/AIDS (2009): 310,000 people -Infant mortality rate: 43.2 deaths/1000 live births
Socioeconomics • Not as productive and industrialized as China • division of labor between formal and informal sectors, and an uneven distribution of wealth and income. • Why?... • stems from the apartheid. Although the transition from a racially based government to a democratic, nonracial government began in the early 1900’s, it wasn’t until 1991 that the apartheid was abolished. • Racial disparities: • black African’s restricted in employment opportunities and limited to low-quality education and health care • white minorities given just the opposite.
Socioeconomics • Unemployment: 25.7% • GDP(2010): $357.3 billion • GDP composition (2010): Agriculture--2%; industry--30.8%; services--66.7%. • Trade (2010): Exports--$85.8 billion (merchandise exports: minerals and metals, motor vehicles and parts, agricultural products.) • South Africa is one of the largest producers of: • platinum • diamonds • Manganese • gold • coal production • Chrome
Politics • The Republic of South Africa: • Multiparty Parliamentary Democracy: -Constitutional powers are shared between the President and the parliament. • Parliament=2 houses • The National Assembly: responsible for drafting the laws of the republic. • Specifically has control over bills relating to monetary matters. • 400 members • The Nation Council of Provinces: Also responsible for drafting the laws of the republic. • 90 members (10 from each province) • Replaced the senate as the 2nd chamber of parliament • The President: Head of State • Jacob Zuma • Elected by the National Assembly • Constitutional responsibilities: • Assigning cabinet portfolios • Signing bills into laws • Commander in chief of the military • Independent Judiciary • Constitutional Court: Interprets/decides constitutional issues. • Supreme Court of Appeal: nonconstitutional matters
South Africa Healthcare system
Health Care. . . • Before (Apartheid) • Black South Africans could not access healthcare • Inequality • absolute insufficient medical facilities and providers in many rural and poorer areas • After • New democratic led to South Africans having . . .” right to access to health care services, including reproductive health care; sufficient food and water; and social security, including, if they are unable to support themselves and their dependents, appropriate social assistance.”
Healthcare Systems Today, South Africa has two parallel systems: Private (20% of population) Public (80% 0f population)
Healthcare Funding The Department of Health has an overall responsibility for healthcare in South Africa, more specially the public sector. Public health consumes 11% of t he government’s total budget. The bulk of health sector funding comes from the South Africa’s National Treasury
Financing… Uniform Patient Fee Schedule(UPFS) National Health Insurance (NHI) The current government is working on national health insurance. - It will serve as a way to make health care more available to those who can not afford it or whose situation restricts of attaining the proper care they need. • The public sectors uses UPFS for billing services • Categorizes patients in three groups: • Full paying patients • Fully subsidized patients • Partially subsidized patients
workforce • There are shortages in the South African workforce. • It is difficult to state categorically how many doctors work in the public and private sectors because some doctors work across both sectors • Many private doctors do sessions in the publics facilities and doctors employed in public facilities also do private work
China & South Africa The Challenges!
Challenges • China - Lack of high-quality patient care-Led to excessive prescriptions • Africa • Apartheid Regime-Whites-Asian-Colored-Blacks
Challenge: China • Lost a focus on patient care due to financial pressure • Economic incentives to over-prescribe drugs or diagnostic services without really improving patient health. • The typical hospital receives less than 10 percent of its income from the government • No universal definition exists to qualified healthcare physicians -70 percent of village doctors had no more than a high school education
Current Reforms In September 2004, a guideline was released restricting prescriptions for seven-day use only, and three days for emergencies. The purpose is to control physicians’ prescription activities to reduce unnecessary prescriptions of drugsWhy its failing it is extremely challenging to enforce compliance to these national regulations, due to China’s huge system
Challenge: South Africa During Apartheid After Apartheid
Challenge: South Africa one physician for every 330 Whites,one physician for every 91,000 Blacks.The life expectancy was 55 years for Blacks, 58 years for Colored, 65 years for Asians, and 70 years for Whites. Blacks had to travel farit was legal to discriminatevirtually no doctors or facilities in the “homelands”
After Apartheid Did it get better? Yes and No After 1994, the new government set priorities to rebuild South African society. These included the improvement of the employment rate and access to quality housing, education, nutrition and health. Programs were developed in order to decrease disparitiesIt is difficult to create an environment of complete equality when a society is branded by a long history of injustice and conflict
Conclusion Only time will tell if both China and South Africa achieved their goals for their citizens-Better access to affordable health care- Equal health care for all