Nourishing Wombs
120 likes | 144 Vues
This study highlights the importance of nutrition interventions during pregnancy to reduce stillbirths and small-for-gestational-age newborns. Key interventions include energy and protein supplementation, iron and folic acid supplementation, deworming, weight gain monitoring, and counseling on nutrition. Various programs exist to support pregnant women with balanced diets and health services. The study evaluates the effectiveness of schemes like Anna Amrutha Hastham and Arogya Laxmi in promoting maternal health. Recommendations include enhancing infrastructure, community audit, and gestational weight gain charts.

Nourishing Wombs
E N D
Presentation Transcript
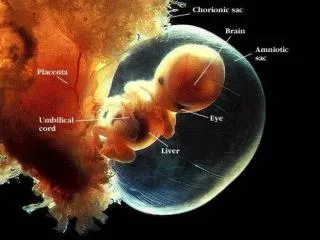
At least 25% of child stunting is attributable to small for gestational age 45,090 maternal deaths during child birth (5 every hour) 27 million Live births 30 million Pregnancies 4.4 million IUGR 5.5 million LBW Calculated based on HMIS 2017 March, MMR=167 & 19% LBW; Danaei et al, 2016
Nutrition-related interventions during pregnancy to reduce of still births and SGA newborns Core Interventions known; programmes exist • Balanced energy and protein supplementation • Iron folic acid and calcium supplementation • Deworming • Weight gain monitoring • Counselling on nutrition, family planning and breastfeeding during ANC contacts • Prevent and treat malarial infections and anemia Supplementary food (ICDS) – 600 Kcal, 18-20 g protein +50% RDA of nine micronutrients Monthly outreach and facility-based antenatal contact points (MoH) CCT- Early pregnancy registration (1000 INR) and at least one ANC after 6 mo (2000 INR) World Health Organization (2016) antenatal care guidelines
Anna AmruthaHastham and ArogyaLaxmi Schemes + Counseling Health services Hot cooked Meal onsite • Supervised Iron folic acid and calcium supplementation • Deworming • ITBN in malaria areas • Gestational weight gain monitoring; MUAC recording • one additional home visit from 20-40th week for women with gestational weight gain<3kgs Fortnightly 24 session calendar (2nd month of pregnancy to 6th month post partum) Rice, dal, vegetables, egg, 200 ml milk. Atleast 40% daily nutritional needs
Rippling effect 2013 102 high-risk blocks • 2015-17 • Andhra Pradesh • Telangana • 2017 • Chhattisgarh • Gujarat • Karnataka • Maharashtra
The Study│ Methods Collaborators: State Government(s), UNICEF, NIN, CESS, Amaltas Consulting Pvt. Ltd Andhra Pradesh Kadapa, Krishna, West Godavari and Vishakhapatnam • Cross-sectional survey • July-November, 2016 • 720 pregnant and lactating women → Receipt of services, food insecurity experiences. → Anthropometry, diet diversity (50% sample) → Dietary recall (15% sample) • Secondary data (Programme MIS) • 1040 (2014, 15, 16) + 710 (2017, Apr-Aug) → pregnancy weight gain → complete receipt of services • Stakeholder interviews (N=252) → what’s working/what’s not/suggestions Telangana Karimnagar, Khammam and Warangal 10 project sites, 120 AWCs
1 Maternal stunting 8% M Maternal severe wasting 4-12% Weight gain between 2nd and 9th month of pregnancy : 8.3–9.7 kg. Pooled for pregnant and lactating beneficiaries
2 Norms and Behaviours Pregnancy – too soon, alcohol in pregnancy % Pooled for pregnant and lactating beneficiaries
3 2. Receipt of Services – The Meal → Average days of consuming scheme’s meal in a month - 17 -23 days → in 60% cases, SHG and family members were motivators → Spot feeding enhanced >=5 maternal dietary diversity (egg, milk) → Dietary energy &protein intake higher on days when the scheme’s meal was consumed. Meal helped meet RDA; prevents severe food insecurity
4 3. Receipt of Services – Health Services and Counseling
5 Stakeholder speak- Areas for improvement • Newly wed young women - for inclusion in high burden geographies. • Budgetary provisions for replenishing infrastructure items • Role and financial partnership of local village organizations • Tag-tracking high-risk pregnancy and minimizing defaulters • Periodic community audit/review of quality of services • MIS usage beyond data retrieval • managerial aspects and individual beneficiary use. • Explore: gestational weight gain charts; package for over and undernourished • Overall with Health –sector – co-reporting , co-planning, co-review
Final statement “Anna Amrutha Hastham and Arogya Laxmi have the potential to become an efficient and cost-effective platform to deliver amalgamated nutrition and non-nutrition interventions outlined in the recent WHO guidelines for a positive pregnancy outcome (WHO, 2016). It could also serve as a workable mechanism for identifying high-risk pregnancies (for example, malnutrition, inadequate pregnancy weight gain, pregnancy-related disease) and facilitating priority referral to the next level of health care. However, it is evident that the non-food component is functioning poorly at ground level and urgent, relevant and perseverant efforts are necessary to ensure efficient convergence with the health system and functionaries”