Download
1 / 45
480 likes | 1.18k Vues
Gastric Dilation and Volvulus Syndrome (GDV). Shanna Jack Margaret Hollis. There is not a single cause found for GDV. Multiple Factors: Dilated stomach Gastric volvulus Dietary factors Increased stress Gastric ligament laxity Conformation- deep chested dogs. Breeds.

E N D
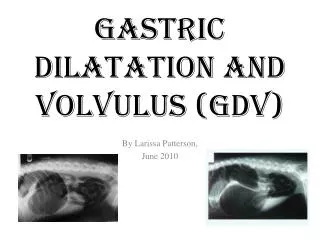
Gastric Dilation and Volvulus Syndrome (GDV) Shanna Jack Margaret Hollis
There is not a single cause found for GDV • Multiple Factors: • Dilated stomach • Gastric volvulus • Dietary factors • Increased stress • Gastric ligament laxity • Conformation- deep chested dogs
Breeds • Great Dane • German Shepard • Standard Poodles • Weimeraners • Saint Bernards • Gordon / Irish Setters • Large Mixed Breeds • Smaller Breeds: Bassett Hound
The Observable Phases of GDV: Phase I: • Pacing, restlessness, salivation & panting • Ineffective Vomiting Attempts (10-20 minute intervals) • Abdomen increased in size & may appear “full”
Phase II: Increased Restlessness Whining Increased salivation, panting Ineffective vomiting attempts every 2-3 minutes Increased heart rate (100 bpm) Abdomen further increased Deep red gums **NEEDS VETERINARY ATTENTION ASAP!! GDV Observable Phases
GDV Observable Phases Phase III: • Gums pale or cyanotic • Dog appears “shaky” when standing, or cannot stand • Abdomen very large • Tachycardia more severe (+100 bpm) • Pulse is weak • Death may be near
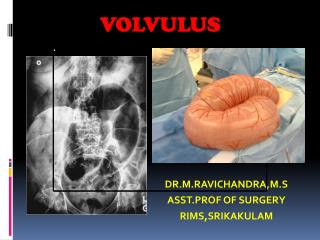
GDV….RADIOGRAPHS!!! Radiographs are: • Necessary in cases of GDV • Needed before surgery • Right lateral is best; ventrodorsal usually is not necessary as this view can add stress
GDV Pathophysiology: • Gastric Distention Gastroesophaeal Angle Change Eructation Impairment • Rotation Stomach Ultimate Duodenum Compression = Prevention of Gastric Emptying
GDV Pathophysiology & Complications • Distention of stomach Decreased venous return of blood to heart Lowered systemic tissue perfusion & shock • Diaphragm compression Decreased ventilation Increase in respiratory rate & decrease in tidal volume
GDV PathophysiologyComplications: • Cardiac arrhythmias • Obstruction of venous outflow & increased intragastric pressure gastric wall edema, anoxia damage to stomach • Often see hemorrhage, necrosis, & mucosal ulcerations; wall of stomach may get necrotic
GDV- Preoperative Care AGGRESSIVE THERAPY!!! • Treat immediately a dog showing signs of GDV • Initially want to treat shock and decrease gastric compression • Stabilizing the patient is the first priority
GDV- Preoperative CareReperfusion injury may play a role in GDV Production of oxygen radicals These radicals lead to lipid peroxidation and cellular death
GDV- Gastric Decompression:Two Main Ways… 1) Orogastric intubation- “Stomach Tube” 2) Needle trocarization
GDV & Gastric Decompression Orogastric intubation: • A lubricated stomach tube is passed to the stomach to relieve gastric compression • Be sure to advance the tube carefully at the gastroesophageal junction. If resistance is found, rotate tube and then advance.
GDV & Gastric Decompression • Passage of the stomach tube into stomach lumen does not mean that there is no gastric rotation!! • Likewise, inability to pass the tube does not confirm rotation of the stomach
GDV & Gastric Decompression Needle Trocarization • An 18 gauge (large bore needle) is used • The stomach wall is against the body wall so other viscera is misplaced, low risk of injury to other tissues
GDV & Treatment of Shock • Intravenous Fluids!!! • Balanced isotonic electrolyte solution given at shock rate (90 ml/kg/hour) • Colloids, hypertonic solution may be indicated • Urinary catheter placed to monitor urine production as an indicator of tissue perfusion (at least 2.0 ml/kg/hour)
GDV & Treatment of Shock • Antibiotics / Glucocorticoids?? • Monitor cardiac arrhythmias with an ECG • It may be helpful to give some patients oxygen
Surgical Correction of Volvulus • Timing depends on patient stabilization • Surgeon’s experience and judgement are important • If gastric necrosis is present, prognosis worsens as time elapses • Usually, surgery occurs within 4-6 hours after presentation
Anesthesia • Neuroleptoanalgesics or narcotics preferred for induction • Maintained with isoflurane or sevoflurane • Nitrous oxide is contraindicated
Surgery • The dog is placed in dorsal recumbency • A standard midline abdominal incision is made from the xiphoid to caudal to the umbilicus
Surgical Anatomy and Rotation • Clockwise rotation of stomach is most common • Most rotations are between 180 and 270 degrees • Occasionally, counterclockwise of 90 degrees is seen • Stomach is rotated about the distal esophagus and tilted cranially
Increased malposition of the stomach with increasing rotation
Repositioning of the Stomach • Manipulate the omentum • Surgeon’s hand enters between the stomach and liver and the stomach is withdrawn caudally • Stomach is grasped to elevate the pylorus and depress the fundus • Stomach gently twisted back into normal position
Complete derotation is determined by palpating and visualizing the cardia and intra-abdominal esophagus • Stomach tube passage can serve as a reference • Easy passage of the tube and lack of tissue folds at the gastroesophageal junction indicate complete derotation
Determining Stomach Viability • Approximately 10% of GDV patients have gastric necrosis • After repositioning the stomach, gastric viability is assessed and devitalized areas are excised by partial gastrectomy
Criteria for Gastric Necrosis • Serosal Color - gray or green • Thickness of stomach wall - thin is bad • Vascular patency
Considerations • Once stomach is repositioned thus relieving venous outflow obstructions, the appearance of the serosa can greatly improve in 5-10 minutes • Small incisions can be made in questionable areas and the appearance of arterial blood indicates probable survival
If any question exists about the viability of an area, that area should be excised
Gastropexy • A technique with the goal of creating a permanent adhesion between the stomach and body wall • Greatly decreases the rate of GDV recurrence • The pyloric antral region is fixed to the adjacent right abdominal wall
Common Procedures of Gastropexy • Right sided Tube Gastrostomy (tube gastropexy) • Incisional Gastropexy • Circumcostal Gastropexy • Belt Loop Gastropexy
Tube Gastropexy • Advantages: - Provides rapid, easy access to the gastric lumen - Relieves post-op gastric distention - Recommended for patients with necrotic gastric tissue Disadvantages: - Potential leakage of gastric contents
Tube Gastropexy • Sutures between the stomach and the body wall maintain the apposition • Omentum develops a water-tight fibrin seal within 4-6 hrs. when it is wrapped around intra-abdominal drains
Incisional Gastropexy • Can be used as a prophylactic procedure in high risk patients • Does not require the aftercare that is involved with tube gastropexy
Initial pyloric antrum incision Matching incision on body wall Suturing of body wall and pyloric antrum
Circumcostal Gastropexy • Popular because it forms a stronger adhesion than two previous methods • Includes a viable muscle flap adhesion and a more proper anatomic placement of the stomach • Disadvantage: Possible rib fracture or creation of pneumothorax
Two 1X4 cm partial thickness gastric flaps are created and are wrapped around either the 11th or 12th costal cartilage
Belt Loop Gastropexy • Modification of circumcostal method • Seromuscular flap is created in the shape of a belt instead of an “I” to eliminate corners and simplify flap passage and suturing • The seromuscular stomach flap is passed around a belt loop of transverse abdominus muscle
GDV- Postoperative Considerations • Closely watch cardiovascular function and electrolyte acid-base status • Do not feed orally for 2-3 days • Give a balanced electrolyte solution IV at 60-120 ml/kg/day
GDV- Postoperative Considerations • Antiarrhythmic medication may be indicated • Lidocaine/ procainamide are most common • Postoperative pain relief with systemic administration of opioid analgesics such as morphine, or oxymorphone
Thank-you!! Any Questions?
References • Aronson, L.R., Brockman, D.J. and D.C. Brown: Gastrointestinal Emergencies. The Veterinary Clinics of North America- Small Animal Practice 30:3, 2000. • Bojrab, Joseph M. Current Techniques in Small Animal Surgery. 4th ed. Williams & Wilkins, Philadelphia. 223-242, 1998 • Glickman LT, Glickman NW, Schellenberg DB, et al. “Incidence of and breed-related factors for gastric dilation-volvulus in dogs.” JAVMA 216:40, 2000. • Matthiesen, David T: Gastric Dilation-Volvulus Syndrome in Textbook of Small Animal Surgery. 2nd ed. W.B. Saunders Co., Philadelphia. 580-591, 1993.