Download
1 / 35
350 likes | 629 Vues
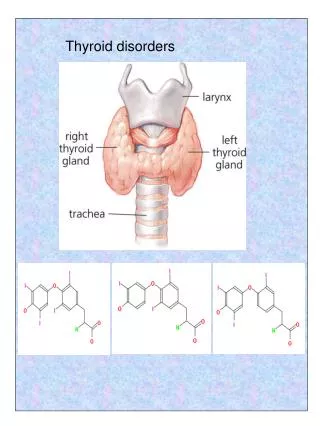
Disorders of Thyroid Function. Dr.nadia hameed. Thyroid Gland Hormones. There are two main hormones produced by the thyroid gland: Thyroxin (T4) and Triiodothyronine (T3).

E N D
Disorders of Thyroid Function Dr.nadiahameed
Thyroid Gland Hormones • There are two main hormones produced by the thyroid gland: Thyroxin (T4) and Triiodothyronine (T3). • Both hormones are derived from the amino acid Tyrosine and contain Iodine that is extracted from the blood. The release of thyroid hormones from the anterior pituitary is regulated by TSH secreted from the anterior pituitary gland.
Disorders of Thyroid Function • An alteration in thyroid function can represent a hypofunctional or a hyperfunctional state. • Disorders of the thyroid may be due to a congenital defect in thyroid development, or they may develop later in life, with a gradual or sudden onset. • Goiter is an increase in the size of the thyroid gland. It can occur in hypothyroid, euthyroid, and hyperthyroid states.
Disorders of Thyroid Function • Goiters may be diffuse, involving the entire gland without evidence of nodularity, or they may contain nodules. • Diffuse nontoxic and multinodular goiters are the result of compensatory hypertrophy and hyperplasia of follicular epithelium from some derangement that impairs thyroid hormone output. • Diffuse goiters usually become nodular. Goiters may be toxic, producing signs of extreme hyperthyroidism or thyrotoxicosis, or they may be nontoxic.
Pathogenesis of Goitre The pathogenetic mechanisms of both forms of goitre can be considered together since nodular goitre is generally regarded as the end-stage of longstanding simple goitre. The fundamental defect is deficient production of thyroid hormones due to various etiologic factors described below, but most common is dietary lack of iodine. Deficient thyroid hormone production causes excessive TSH stimulation which leads to hyperplasia of follicular epithelium as well as formation of new thyroid follicles. Cyclical hyperplastic stage followed by involution stage completes the picture of simple goitre. Repeated and prolonged changes of hyperplasia result in continued growth of thyroid tissue while involuted areas undergo fibrosis, thus completing the picture of nodular goitre
Hypothyroidism • Hypothyroidism can occur as a congenital or an acquired defect. Congenital hypothyroidism develops prenatally and is present at birth. Acquired hypothyroidism develops later in life because of primary disease of the thyroid gland or secondary to disorders of hypothalamic or pituitary origin. • Congenital hypothyroidism: is a common cause of mental retardation. It affects approximately 1 of 5000 infants.
Hypothyroidism • Hypothyroidism in the infant may result from a congenital lack of the thyroid gland or from abnormal biosynthesis of thyroid hormone or deficient TSH secretion. • With congenital lack of the thyroid gland, the infant usually appears normal and functions normally at birth because of hormones supplied in utero by the mother.
Hypothyroidism • There may be respiratory difficulties and a hoarse cry, due in part to the enlarged tongue; feeding difficulties, especially sluggishness, lack of interest, and choking during nursing; an enlarged abdomen; and an umbilical hernia. The manifestations of untreated congenital hypothyroidism are referred to as cretinism. However, the term does not apply to the normally developing infant in whom replacement thyroid hormone therapy was instituted shortly after birth.
Hypothyroidism • Thyroid hormone is essential for normal growth and brain development, almost half of which occurs during the first 6 months of life. If untreated, congenital hypothyroidism causes mental retardation and impairs physical growth. Long-term studies show that closely monitored T4 supplementation begun in the first 6 weeks of life results in normal intelligence. Fortunately, many countries throughout the world now routinely screen newborns for hypothyroidism, providing the means for early diagnosis and treatment.
Hypothyroidism • The screening test involves taking a drop of blood from the infant’s heel and sending it to a central laboratory, where it is analyzed for T4 or TSH. Screening is done 24 to 48 hours after birth, usually in the hospital nursery. • Transient congenital hypothyroidism has been recognized more frequently since the introduction of neonatal screening. It is characterized by high TSH levels and low or normal thyroid hormone levels.
Hypothyroidism • The fetal and infant thyroids are sensitive to iodine excess. Iodine crosses the placenta and mammary glands and is readily absorbed by infant skin. • Transient hypothyroidism may be caused by maternal or infant exposure to substances such as povidone-iodine used as a disinfectant (i.e., vaginal douche or skin disinfectant in the nursery). Antithyroid drugs such as propylthiouracil and methimazole can cross the placenta and in large doses will impair fetal thyroid function.
Hypothyroidism • Acquired Hypothyroidism: Hypothyroidism in older children and adults causes a general slowing down of metabolic processes and myxedema.
Hypothyroidism • Myxedema implies the presence of a nonpitting mucous type of edema caused by an accumulation of a hydrophilic mucopolysaccharide substance in the connective tissues throughout the body. • The hypothyroid state may be mild, with only a few signs and symptoms, or it may progress to a life-threatening condition called myxedematous coma. It can result from destruction or dysfunction of the thyroid gland (i.e., primary hypothyroidism), as a secondary disorder caused by impaired pituitary function, or as a tertiary disorder caused by a hypothalamic dysfunction.
Hypothyroidism • Primary hypothyroidism is much more common than secondary (and tertiary) hypothyroidism. It may result from thyroidectomy (i.e., surgical removal) or ablation of the gland with radiation. Certain goitrogenic agents, such as lithium carbonate (used in the treatment of manicdepressive states), and the antithyroid drugs propylthiouracil and methimazole in continuous dosage can block hormone synthesis and produce hypothyroidism with goiter.
Hypothyroidism • Large amounts of iodine (i.e., ingestion of kelp tablets or iodide-containing cough syrups, or administration of iodide-containing radiographic contrast media or the cardiac drug amiodarone, which contains 75 mg of iodine per 200-mg tablet) also can block thyroid hormone production and cause goiter, particularly in persons with autoimmune thyroid disease. • The most common cause of hypothyroidism is Hashimoto thyroiditis, an autoimmune disorder in which the thyroid gland may be totally destroyed by an immunologic process. It is the major cause of goiter and hypothyroidism in children and adults. Hashimoto thyroiditis is predominantly a disease of women, with a female-to-male ratio of 5:1.
Hypothyroidism • Although the disorder usually causes hypothyroidism, a hyperthyroid state may develop midcourse in the disease. The transient hyperthyroid state is caused by leakage of preformed thyroid hormone from damaged cells of the gland. Subacute thyroiditis, which can occur in up to 10% of pregnancies postpartum (postpartum thyroiditis), also can result in hypothyroidism.
Hypothyroidism • Hypothyroidism may affect almost all body functions. The manifestations of the disorder are related largely to two factors: the hypometabolic state resulting from thyroid hormone deficiency, and myxedematous involvement of body tissues. The hypometabolic state associated with hypothyroidism is characterized by a gradual onset of weakness and fatigue, a tendency to gain weight despite a loss of appetite, and cold intolerance.
Hypothyroidism • As the condition progresses, the skin becomes dry and rough and the hair becomes coarse and brittle. Reduced conversion of carotene to vitamin A and increased blood levels of carotene may give the skin a yellowish color. The face becomes puffy with edematous eyelids, and there is thinning of the outer third of the eyebrows. Fluid may collect in almost any serous cavity and in the middle ear, giving rise to conductive deafness.
Hypothyroidism • Gastrointestinal motility is decreased, producing constipation, and abdominal distention. • Delayed relaxation of deep tendon reflexes and bradycardia are sometimes noted. • Central nervous system involvement is manifested in mental dullness, lethargy, and impaired memory. • Although the myxedematous fluid is usually most obvious in the face, it can collect in the interstitial spaces of almost any body structure and is responsible for many of the manifestations of the severe hypothyroid state. The tongue is often enlarged, and the voice becomes hoarse and husky.
Hyperthyroidism • Hyperthyroidism is the clinical syndrome that results when tissues are exposed to high levels of circulating thyroid hormone. • In most instances, hyperthyroidism is due to hyperactivity of the thyroid gland. • The most common causes of hyperthyroidism are Graves disease, which is accompanied by ophthalmopathy (or dermopathy) and diffuse goiter. • Other causes of hyperthyroidism are multinodular goiter, adenoma of the thyroid, and thyroiditis. • Iodine-containing agents can induce hyperthyroidism as well as hypothyroidism. Thyroid crisis, or storm, is an acutely exaggerated manifestation of the thyrotoxic state.
Hyperthyroidism • Many of the manifestations of hyperthyroidism are related to the increase in oxygen consumption and use of metabolic fuels associated with the hypermetabolic state, as well as to the increase in sympathetic nervous system activity that occurs. • Other manifestations include tachycardia, palpitations, shortness of breath, excessive sweating, muscle cramps, and heat intolerance. The person appears restless and has a fine muscle tremor. • The hair and skin usually are thin and have a silky appearance. About 15% of elderly individuals with new-onset atrial fibrillation have thyrotoxicosis.
Hyperthyroidism • Even in persons without exophthalmos (i.e., bulging of the eyeballs seen in ophthalmopathy), there is an abnormal retraction of the eyelids and infrequent blinking such that they appear to be staring.
Graves Disease • Graves disease is a state of hyperthyroidism, goiter, ophthalmopathy, or, less commonly, dermopathy. • The onset usually is between the ages of 20 and 40 years, and women are five times more likely to develop the disease than men. • Graves disease is an autoimmune disorder characterized by abnormal stimulation of the thyroid gland by thyroid-stimulating antibodies (TSH-receptor antibodies) that act through the normal TSH receptors.
Graves Disease • It may be associated with other autoimmune disorders such as myasthenia gravis and pernicious anemia. The disease is associated with human leukocyte antigen (HLA)-DR3 and HLA-B8, and a familial tendency is evident.
Graves Disease • The ophthalmopathy, which occurs in up to one third of persons with Graves disease, is thought to result from a cytokine-mediated activation of fibroblasts in orbital tissue behind the eyeball. Humoral autoimmunity also is important; an ophthalmic immunoglobulin may exacerbate lymphocytic infiltration of the extraocular muscles.
Graves Disease • The ophthalmopathy of Graves disease can cause severe eye problems, including abnormal positioning of the extraocular muscles resulting in diplopia; involvement of the optic nerve, with some visual loss; and corneal ulceration because the lids do not close over the protruding eyeball (due to the exophthalmos).
Thyrotoxicosis • Thyroid storm, or crisis, is an extreme and life-threatening form of thyrotoxicosis, rarely seen today because of improved diagnosis and treatment methods. • When it does occur, it is seen most often in undiagnosed cases or in persons with hyperthyroidism who have not been adequately treated.
Thyrotoxicosis • It often is precipitated by stress such as an infection (usually respiratory), diabetic ketoacidosis, physical or emotional trauma, or manipulation of a hyperactive thyroid gland during thyroidectomy. • Thyroid storm is manifested by a very high fever, extreme cardiovascular effects (i.e., tachycardia, congestive failure, and angina), and severe CNS effects (i.e., agitation, restlessness, and delirium). The mortality rate is high.
Thyrotoxicosis • Thyroid storm requires rapid diagnosis and implementation of treatment. Peripheral cooling is initiated with cold packs and a cooling mattress. For cooling to be effective, the shivering response must be prevented. • General supportive measures to replace fluids, glucose, and electrolytes are essential during the hypermetabolic state. • A β-adrenergic blocking drug, such as propranolol, is used to block the undesirable effects of T4 on cardiovascular function.