THE THYROID GLAND AND DISORDERS OF THYROID FUNCTION
1.06k likes | 1.72k Vues
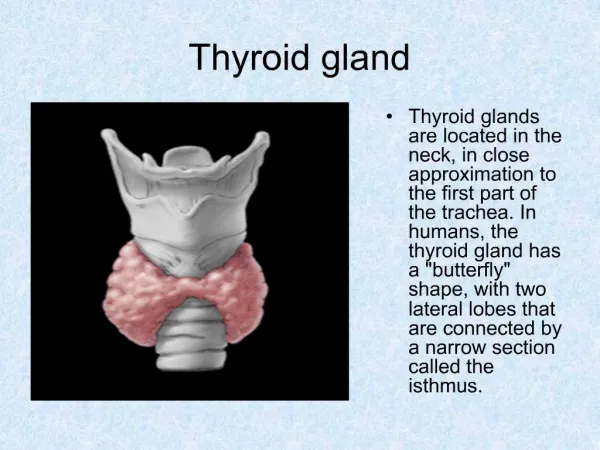
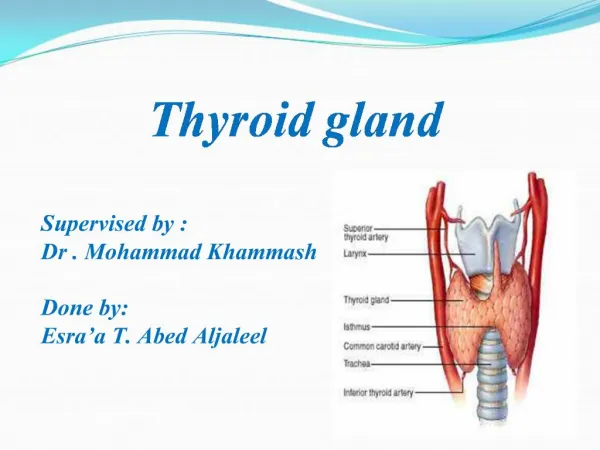
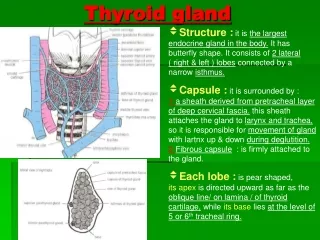
THE THYROID GLAND AND DISORDERS OF THYROID FUNCTION. Dr B Onyenekwe. THYROID GLAND. The largest endocrine gland, located in the anterior neck, consists of two lateral lobes connected by a median tissue mass called the isthmus

THE THYROID GLAND AND DISORDERS OF THYROID FUNCTION
E N D
Presentation Transcript
THE THYROID GLAND AND DISORDERS OF THYROID FUNCTION Dr B Onyenekwe
THYROID GLAND • The largest endocrine gland, located in the anterior neck, consists of two lateral lobes connected by a median tissue mass called the isthmus • adult normal gland weighs 15-20 g in an iodine replete population. • Composed of follicles that produce and store the glycoprotein thyroglobulin • Colloid (thyroglobulin + iodine) fills the lumen of the follicles and is the precursor of thyroid hormone • Interspersed between the thyroid follicles are the parafollicular C cells which secrete calcitonin.
Iodine metabolism • Iodide is required for thyroid hormone synthesis. • The major sources of dietary iodide are both food and water or iodized water or food products, such as bread and salt, medications, diagnostic agents, and dietary supplements are also potential sources of iodine. • The range of iodine intake in adults across areas of the world in which iodine deficiency is not severe enough to impair thyroid hormonogenesis varies from 50 to 1000µg/day.
Iodine metabolism • Iodine is almost completely absorbed in the gastrointestinal tract where it enters the inorganic iodide pool in the extracellular fluid with small contribution from iodide released following the deiodination of thyroid hormones in peripheral tissues and the leak of inorganic iodide from the thyroid gland. • Iodide clearance from the extracellular pool is via the thyroid and the kidney. • The major iodine pool in the body is thyroglobulin in the colloid within the follicular lumen.
Thyroid Hormone • Thyroid hormone – the body’s major metabolic hormone • Consists of two closely related iodine-containing compounds • T4 – thyroxine; has two tyrosine molecules plus four bound iodine atoms • T3 – triiodothyronine; has two tyrosines with three bound iodine atoms
Thyroid hormone action • Thyroid hormone act trough interaction with nuclear receptors for T3 in target cells. • All thyroid hormone-dependent processes are initiated by the interaction of the thyroid hormone-thyroid hormone receptor complex with the DNA sequence of the thyroid hormone response element influencing a number of metabolic processes by their action on a variety of enzymes; the metabolism of substrates, vitamins, and minerals; the secretion and degradation rates of virtually all other hormones and the response of their target tissues to them.
Effects of thyroid hormones Effects of thyroid hormones on metabolic processes • Metabolic rate: increased BMR • Calorogenic: increased heat production (oxidative metabolism) • Sympathomimetic: Fight or Flight • Cardiovascular: increased heart rate and contractions • Growth: essential for normal growth of skeletal system (permissive or synergistic with GH, insulin-like growth factors), CNS, ANS • Nervous system: development and maturation
Synthesis of Thyroid Hormone • Thyroglobulin is synthesized and discharged into the lumen • Iodides (I–) are actively taken into the cell, oxidized to iodine (I2) by thyroid peroxidase and released into the lumen • Iodine attaches to tyrosine, mediated by peroxidase enzymes, forming T1 (monoiodotyrosine, or MIT), and T2 (diiodotyrosine, or DIT) (iodide organification) • Iodinated tyrosines link together to form T3 and T4 (coupling) • Colloid is then endocytosed and combined with a lysosome, where T3 and T4 are cleaved and diffuse into the bloodstream
Thyroid hormone transport and metabolism • T4 and T3 bind to thyroxine-binding globulins (TBGs 75%)thyroxine-binding prealbumin, transthyretin, and, to a smaller extent, by albumin. Only about 0.04 % of T4 and 0.4 % of T3 circulate in the unbound state (free). • T4 is the most abundant iodothyronines circulating in the plasma, and is the only one that arises solely by direct secretion from the thyroid gland.
Thyroid hormone transport and metabolism • Both bind to target receptors, but T3 is ten times more active than T4 • Peripheral tissues convert T4 to T3 (the source of most T3) • Regulation is by negative feedback • Hypothalamic thyrotropin-releasing hormone (TRH) can overcome the negative feedback
Thyroid hormone transport and metabolism • The most important pathway for the metabolism of T4 is its conversion to the biologically active hormone T3. • The remaining deiodination reactions of T4 and of T3 all lead to the generation of inactive products catalyzed by deiodinase. • A number of factors impair the peripheral conversion of T4 to T3.
Regulation of thyroid function • Extrathyroidal (TSH) mechanism: TSH is the major regulator of thyroid structure and function by the classical feedback control system Its secretion, in turn, is regulated by thyrotropin releasing hormone (TRH) from the hypothalamus which stimulates the pituitary thyrotroph to release and later synthesize TSH. • Intrathyroidal mechanism Fluctuations in hormone secretion are prevented in part by the large intraglandular store of hormone which buffers the effects of acute increases or decreases in hormone synthesis. Autoregulatory mechanisms within the gland maintain the constancy of the intraglandular hormone pool.
Laboratory investigation of structure and function • Assessment of a patient with suspected thyroid disease is designed to evaluate: (1) hormone over- or under-production; and (2) the cause of the underlying disorder? • Thyroid hormones measurement • Sensitive immunoassay for the measurement of total serum T4 and T3 to establish normal ranges for circulating thyroid hormones • Total T4 discriminates well between hyperthyroidism, hypothyroidism, and the euthyroid state. • T3 levels are often within the normal range in the hypothyroid, may rise before changes in total T4 levels are detectable in the hyperthyroid patient.
Laboratory investigation of structure and function Measurement of free thyroid hormone • Thyroglobulin Thyroglobulin is present at low levels (up to 30pmol/l) in the circulation of normal individuals. The major clinical value mgt of patients with differentiated thyroid carcinoma. • Thyroid gland iodine metabolism by theuse of a tracer dose of a radioactive isotope of iodine and measurement of its fractional uptake by the gland using a γ-scintillation counter over the area of the thyroid 24 h later. • The efficiency of thyroid organification is examined using the discharge of radioactive iodine from the thyroid in response to the administration of potassium perchlorate, the perchlorate discharge test.
Laboratory investigation of structure and function Hypothalamic-pituitary-thyroid axis • Measurement of plasmaTSH Using sensitive third-generation immunometric assays, allows the diagnosis of primary hypothyroidism to be made with confidence [TSH]. • Symptomatic primary hyperthyroidism is accompanied almost without exception by TSH levels below 0.01 mU/l. • With plasmaTSH it is also possible to discriminate between hypothyroidism of thyroid origin and that due to diseases of the hypothalamic-pituitary axis making it needless to perform TRH infusion tests or thyroid suppression tests.
Laboratory investigation of structure and function • Thyroid imaging • Radionuclide scanning is based on the principle that isotopically labelled materials accumulate differentially in thyroid tissue and the detection and quantification of this information is transformed into a visual display. This allows the localization of functioning and non-functioning thyroid tissue. A number of isotopes of iodine and 99Tcm pertechnetate have been used.
PATTERN: NORMAL LOCALIZATION “Trapping” in salivary gland = Tc99m < I-123 Asymetric size : normal variaton
Graves’ diseaseIsthmus, pyramidal lobe :visible in Graves’ diseasebut, seen other conditions causing enlargement.
Solitary “hot” nodule Dx. : autonomous adenoma“Hot” nodules are almost always benign
Laboratory investigation of structure and function Ultrasonography can demonstrate • diffuse or localized enlargement of the gland • provide objective assessments of change in size. • The sensitivity of the technique allows detection of nodules which are not clinically palpable. • The major role of ultrasonography is in the differentiation of cystic from solid lesions in the thyroid and when a solitary nodule can be shown to be purely cystic this considerably reduces the likelihood of it being malignant
Laboratory investigation of structure and function Peripheral effects of thyroid hormones • The best established and validated (but also most cumbersome) investigation is the basal metabolic rate. • The speed of relaxation of the Achilles tendon reflex, which is prolonged in hypothyroidism and shortened in hyperthyroidism. • The serum cholesterol is usually elevated in hypothyroidism and decreased in hyperthyroidism and the serum creatinine phosphokinase may be increased in the hypothyroid state. • Fine-needle aspiration biopsy • Fine-needle aspiration biopsy is used for solitary cold nodules coupled with cytological examination
Thyroid autoantibodies • Thyroglobulin Antibodies present in 80 per cent of patients with autoimmune thyroiditis goitrous or atrophic, and in some 35 per cent of patients with newly diagnosed hyperthyroid Graves' disease. Seems not to have any role in the pathogenesis of autoimmune thyroid disease • Thyroid Peroxidase Antibodies present in almost all those with autoimmune thyroid disease at some stage in the disease process. • Thyroid Stimulating Hormone Receptor Antibodies are present in all patients with hyperthyroid Graves' disease prior to treatment
DISORDERS OF THE THYROID • Patients presenting with disorders of the thyroid may present with symptoms which relate to[1] hyperthyroidism, hypothyroidism, to enlargement of the gland, and/or to the [2]complications of Graves' disease. [3]Local symptoms including pain or compression of adjacent structures. • Risk assessment • Evidence of possible exposure to ionizing radiation, of iodide ingestion in the form of food preparations, or of iodine-containing medications, such as amiodarone, lithium carbonate etc which may affect thyroid function is assessed.
DISORDERS OF THE THYROID • Risk assessment • Origin or residence in areas of endemic low dietary iodide intake should be sought. A family history of goitre, altered thyroid function, and a personal and family history [histories of insulin-dependent diabetes, pernicious anaemia, vitiligo, and myasthenia gravis], may be helpful. • Examination of the neck should be performed to assess the size and consistency of the gland and the presence or absence of nodules within it, whether the enlargement is diffuse or nodular and the size of individual nodules.
DISORDERS OF THE THYROID • Examination • The thyroid may be tender or, rarely, exceedingly painful to touch • Search the neck for enlargedlocal lymph nodes. Auscultation over the thyroid in patients with hyperthyroidism, • Transillumination of large nodules within the thyroid. • A retrosternal goitre; may give a positive Pemberton's sign, displacement of the trachea and inspiratory stridor. Hoarseness of the voice, consider possible involvement of the recurrent laryngeal nerve, most usually by a malignant thyroid lesion.
THYROID HORMONE EXCESS • Thyrotoxicosis is the clinical syndrome that results when tissues are exposed to high levels of circulating thyroid hormone. In most instances this situation arises as a result of hyperactivity of the thyroid gland (hyperthyroidism). The prevalence of this disorder is approximately 20 per 1000 in females and 2 per 1000 in males • Causes of hyperthyroidism • Common: Graves' disease (diffuse toxic goitre); Toxic multinodular goiter; Toxic solitary adenoma; • Thyroiditis sub-acute, viral, de Quervain's, silent, painless, postpartum
THYROID HORMONE EXCESS • Uncommon: Hyperthyroid phase of Hashimoto's thyroiditis, Neonatal hyperthyroidism; Iodine-induced ;Thyrotoxicosis factitia; Hydatidiform mole; choriocarcinoma; TSH-secreting pituitary adenoma; Metastatic thyroid carcinoma (follicular; ), Struma ovarii (thyroid-tissue-containing teratoma) • PRESENTATION • Patients can present with a wide variety of symptoms and accompanying physical signs. The presentation of the disease depends on its severity, duration, aetiology, age of the patient, and the presence or absence of disease in other organs. It may present gradually, which is usual, or acutely.
Clinical features associated with hyperthyroidism General Heat intolerance Sweating Fatigue Apathy Tremor Diffuse goitre Nodular goitre Cardiovascular Palpitation Dyspnoea Angina Tachycardia Atrial fibrillation Heart failure Gastrointestinal Weight loss despite increased appetite Diarrhoea, steatorrhoea Vomiting THYROID HORMONE EXCESS
Genitourinary Polyuria and polydipsia Amenorrhoea Infertility Neuromuscular Fatiguability Restlessness Muscle weakness; proximal Choreoathetosis Hypokalaemic periodic paralysis Myasthenia gravis Psychiatric Irritability Nervousness Agitation Emotional lability Psychosis Ocular Lid lag/lid retraction Ophthalmopathy THYROID HORMONE EXCESS
Ocular Lid lag/lid retractionLid retraction,[ stare] can occur in any form of thyrotoxicosis [sympathetic overactivity.] Specific eye signs comprise Graves' ophthalmopathy [thyroid-associated ophthalmopathy] It occurs in the absence of Graves' disease in 10%; within the year before or after the diagnosis in 75%; precede or follow thyrotoxicosis by several years, [euthyroid ophthalmopathy] Unilateral signs are found in up to 10% Earliest manifestations usually; grittiness, eye discomfort, and excess tearing Proptosis periorbital edema, scleral injection, and chemosis are also frequent. 5 to 10% of patients have diplopia
THYROID HORMONE EXCESS • NO SPECS scheme • Scoring system used to gauge the extent and activity of the orbital changes in Graves' disease. • 0 = No signs or symptoms • 1 = Only signs (lid retraction or lag), no symptoms • 2 = Soft tissue involvement (periorbital edema) • 3 = Proptosis (>22 mm) • 4 = Extraocular muscle involvement (diplopia) • 5 = Corneal involvement • 6 = Sight loss
THYROID HORMONE EXCESS • Thyroid dermopathy • Occurs in <5% of patients with Graves' disease • Almost always occurs in the presence of moderate or severe ophthalmopathy. • Most frequent over the anterior and lateral aspects of the lower leg (pretibial myxedema), • The typical lesion is a noninflamed, elevated, firm, nonpitting, localized thickening [ indurated plaque] with an "orange-skin" appearance. • Thyroid acropachy refers to a form of clubbing found in <1% of patients with Graves' disease It is very strongly associated with thyroid dermopathy
THYROID HORMONE EXCESS • Hair thinning, Onycholysis, Vitiligo, • Weight gain occurs in 5 to 10% of patients • Bone: bone resorption leads to osteopenia in long-standing thyrotoxicosis; mild hypercalcemia occurs in up to 20% of patients, but hypercalcuria is more common • Confirmation of the diagnosis requires laboratory assessment. Hyperthyroidism is indicated by elevated concentrations of free or total T4 and T3 in the presence of an undetectable level of TSH. Uncommonly, T3 values are elevated despite normal T4 values (T3 toxicosis).
THYROID HORMONE EXCESS • The presence of thyroid autoantibodies in conjunction with a diffuse goitre, and evidence of increased uptake in an isotope scan makes the cause of the hyperthyroidism almost certainly due to Graves' disease. • A radioisotope scan also allows the demonstration of a solitary toxic nodule or of a toxic multinodular goitre. In these last two situations thyroid autoantibodies will not be detected
THYROID HORMONE EXCESS • Graves' disease • is the most common cause of hyperthyroidism • Is characterized by a diffusely enlarged thyroid gland, hyperthyroidism, ophthalmopathy and, uncommonly, dermopathy (pretibial myxoedema). • It is an organ-specific autoimmune disease with a strong familial predisposition, occurring much more commonly in females and with a peak incidence between the ages of 20 and 40 years. • It is associated with other organ-specific autoimmune diseases. Lymphocytic infiltration of the thyroid gland is a hallmark of the autoimmune process. • .
THYROID HORMONE EXCESS • The pathogenetic process finally leading to hyperthyroidism depends on the presence TSH receptor antibodies which are usually of the IgG1 subclass • TOXIC MULTINODULAR GOITRE • Hyperthyroidism in this setting usually occurs in an older age group with a long-standingmultinodular goiter. Hyperthyroidism may be precipitated by the administration of iodides [iodine induced hyperthyroidism-IIH]. Thyroid hormone overproduction is usually much less marked than occurs in Graves' disease, so that the clinical presentation is less dramatic
THYROID HORMONE EXCESS • TOXIC SOLITARY ADENOMA • Less than 2 per cent of patients presenting with hyperthyroidism are found to have a solitary toxic adenoma as the cause. These solitary nodules occur in a younger age group, usually in patients in their 30s and 40s. The disorder is usually caused by a single palpable nodule. • THYROIDITIS • Subacute thyroiditis, also known as granulomatous giant cell or de Quervain's thyroiditis, is due to a viral infection of the thyroid gland, often following an upper respiratory tract infection. The disease is uncommon.
THYROID HORMONE EXCESS • Silent thyroiditis (painless) • Hyperthyroidism may also occur in. • The thyroid may be enlarged during the disease but is not tender to touch. • The disease is almost certainly autoimmune in origin, with the characteristic lymphocyticinfiltration of the gland, the presence of antithyroid antibodies and HLA associations
DIFFERENTIALS Graves disease: diffusely enlarged thyroid, thyroid bruits, ophthalmology, pretibial myxedema, and the presence of TSIs. Multinodular toxic goiter: elderly individuals and multiple nodules palpated or observed after thyroid scans. Toxic adenoma: solitary palpable nodule and a "hot" nodule observed after a thyroid scan Subacute thyroiditis: history of antecedent respiratory tract infection, neck tenderness, elevated sedimentation rate, low or absent radioactive iodine uptake, and a self-limited course.
DIFFERENTIALS Silent thyroiditis: Special features include painless thyroiditis, which may be seen in postpartum women (postpartum thyroiditis); a self-limited course; and low radioiodine uptake. Iodide-induced thyrotoxicosis: patients with a history of nodular thyroid disease who have been exposed to iodine-containing contrast agents or drugs such as amiodarone or iodine supplementation of the diet.
TREATMENT • Directed towards controlling the hyperthyroidism by: • inhibiting thyroid hormone synthesis and release by means of antithyroid drugs or • reducing the bulk of the thyroid tissue by either partial thyroidectomy or radio-iodine administration. Antithyroid drugs • The major group of drugs used for the treatment of hyperthyroidism is the thionamides.Carbimazole propylthiouracil or methimazole, the active metabolite of carbimazole, are the agents of choice.
Antithyroid drugs • Allinhibit both oxidation and organification, thus leading to a state of intrathyroidal iodine deficiency and inhibition of thyroid hormone synthesis. • In addition, propylthiouracil inhibits the conversion of T4 to T3 in the periphery. • All are weakly immunosuppressive and this effect may contribute to the control of Graves' disease by reducing the levels of TSH receptor antibodies. • Carbimazole is usually begun at a dose of 40mg daily.
Antithyroid drugs • Improvement in symptoms and thyroid function by 4 to 8 weeks after commencing therapy. • Subsequent management is either by titration of the dose of carbimazole against the clinical and biochemical response. • Alternatively, a blocking and replacement regimen can be used, in which carbimazole is maintained at a dose of 40mg once daily with thyroxine (50-150 µg/day) being added once thyroid function is under control.
Antithyroid drugs • Following such treatment with carbimazole in a blocking and replacement regimen for 6 to 12months, between a third and half the patients achieve lasting remission. • Factors that predict the likelihood of long-term remission at the end of a course of drug therapy are a small goitre, a decrease in goitre size during treatment, a normal serum TSH level and disappearance of TSH receptor antibody activity from the serum.
Partial thyroidectomy • Surgery is exceedingly effective in relieving hyperthyroidism. • Patients should be made euthyroid prior to surgery by the use of carbimazole for at least 2 to 3months before the operation and by the addition of Lugol's solution (0.1-0.3 ml three times a day) for 10days immediately prior to the operation. • With long follow-up, up to half the patients may go on to develop hypothyroidism.