Download
1 / 1
30 likes | 185 Vues
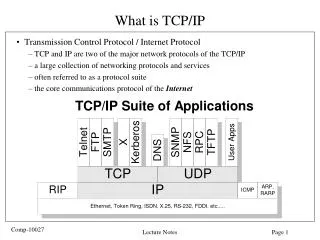
Compliance with Severe Sepsis Protocol: Impact on Patient Outcomes Lisa Hurst RN BSN CCRN and Kim Raines RN CCRN. Background. Purpose. Findings. Discussion. The time to treatment (blood cultures, antibiotics, lactate) is significantly longer than recommended.

E N D
Compliance with Severe Sepsis Protocol: Impact on Patient Outcomes Lisa Hurst RN BSN CCRN and Kim Raines RN CCRN Background Purpose Findings Discussion • The time to treatment (blood cultures, antibiotics, lactate) is significantly longer than recommended. • Some patients did not have blood cultures or lactate levels and therefore important measures of sepsis diagnosis were not available (these data points assigned 0 value in calculations for treatment chart). • Tests not consistently ordered/drawn ‘stat’, ABGs obtained without lactate. • Critical Care Managers (CCM) are experts in severe sepsis management. CCM consult is ordered on the protocol at UPMC Hamot. 44% of patients were seen by CCM. • The average time to first CCM order was 9.3 hours. This means that patients were not seen by the experts within the critical resuscitation window of 6 hours. • Perhaps this partially explains the low protocol initiation (10%) on patients seen by CCM. • Consistent use of a standardized protocol “ensures implementation of evidence based guidelines, decreases variability in management among clinicians…and monitors quality of care” (Moore, 2009). Limitations: • Some regional patients were transferred after the initial critical phase, which may have influenced the decision to initiate the protocol, and thus compliance time. • In patients with SIRS that deteriorated to severe sepsis, data was not collected on the time between vital sign change and physician response. • All patients in this study met criteria for severe sepsis according to the disease continuum definition at the time of diagnosis. There were significant variations in documentation of diagnosis of severe sepsis among clinicians. • Small sample size limits generalization of findings. • In 2001, the European Society of Intensive Care Medicine (ESICM), Society of Critical Care Medicine (SCCM), and the International Sepsis Forum (ISF) developed the Surviving Sepsis Campaign. • The purpose of this initiative was to improve diagnosis, management, and treatment of sepsis. • This international effort produced the Sepsis Management Bundles, which are guidelines updated periodically by the Campaign. • These bundles outline Early Goal Directed Therapy(EGDT) interventions which studies have proven decrease organ dysfunction and improve clinical outcomes and functional status (Zubrow, 2008). • Established at UPMC Hamot as the Severe SepsisProtocol, the interventions include blood cultures and antibiotics within one hour, fluid resuscitation and vasopressors if necessary, for hemodynamic stability. Lactate and PreSep (ScVO2) catheter insertion for monitoring tissue perfusion must be completed within six hours of diagnosis. The purpose of this study is to establish the current level of medical compliance with the Severe Sepsis Protocol at UPMC Hamot. • *Dx=diagnosis Cx=blood cultures Lact=lactate Abx=antibiotics • Recommended time: • Blood cultures drawn, 1 hour • Antibiotics administered, 1 hour • Lactate levels drawn, 6 hours Regardless of the source, severe sepsis is a syndrome that is characterized by systemic inflammatory response syndrome (SIRS) with a source of infection, one or more organ involvement, and hemodynamic instability. Resuscitation Bundle (Dellinger, 2008) (To be accomplished as soon as possible and scored over first 6 hours): • Serum lactate measured • Blood cultures obtained prior to antibiotics administered • Perform imaging studies promptly to find source • Administration of broad-spectrum antibiotics within 1 hour of diagnosis of septic shock and severe sepsis without septic shock • For hypotension and/or lactate > 4 mmol/L Deliver an initial minimum of 20 mL/kg of crystalloid (or colloid equivalent) • Apply vasopressors for hypotension not responding to initial fluid resuscitation to maintain MAP > 65 mmHg. • For persistent hypotension despite initial fluid resuscitation (septic shock) and/or lactate > 4 mmol/L • Achieve CVP of 8-12 mmHg & MAP > 65 mmHg & UO > 0.5mL/kg/hr • Achieve ScvO2 of> 70% or SvO2 > 65%. • if ScvO2 not > 70% consider blood or dobutamine Methods The Severe Sepsis Bundles: Surviving Sepsis Campaign/IHI* • The UPMC Hamot Institutional Review Board (IRB) approved retrospective chart reviews to identify 50 patients with a diagnosis of severe sepsis or sepsis with organ dysfunction. Patients were hospitalized at UPMC Hamot between 1/1/10 and 12/31/10. • The following data was collected: • age • source of sepsis • length of stay • mortality/functional status at time of admission and discharge Time of: • admission • severe sepsis order set • blood cultures, lactate, and antibiotics • post severe sepsis diagnosis • first CCM order obtained post severe sepsis • diagnosis • PreSep (ScVO2) catheter insertion • ScVO2 value ≥ 70% noted • The time of diagnosis was determined by physician progress notes or by patient presentation to ICU or ER. • 22 patients (44%) had CCM consult • 9 patients (18%) placed on protocol • 5 patients (10%) protocol + CCM consult • 8 patients (16%) received PreSep • (ScVO2) catheter • 6 patients (12%) received PreSep (ScVO2) + CCM consult • The catheter provides continuous valuable data about organ perfusion that guides interventions according to the Severe Sepsis Protocol. Recommendations • Additional studies are needed to measure knowledge of nurses after provision of comprehensive education. • Formation of Sepsis Alert Teams have been demonstrated to improve outcomes and decrease sepsis-related mortality (Zubrow, 2008). • Sepsis Screening Tools have been shown to improve outcomes because early identification and EGDTdecrease organ involvement and sepsis related mortality (Moore, 2009). • Education at regional referral sites of signs and symptoms of severe sepsis and use of the protocol may promote EGDT. • Studies show that protocol compliance reduces organ dysfunction and mortality. Could we, at UPMC Hamot, improveProtocol compliance and therefore, functional status at discharge? This could be a topic for future research after implementation of evidence based practice changes such as: sepsis alert team, sepsis screening tool, and education of medical staff. References • 56% of patients discharged to SNIF/Rehab • 22% of patients died • 22% discharged home • 78% of patients came from home; only 22% were able to return directly home due to change in functional status • Dellinger, R.P., et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2008. Crit Care Med. 2008;36:296-327. • Gao, F., et al. The impact of compliance with 6-hour and 24-hour sepsis bundles on hospital mortality in patients with severe sepsis: a prospective observational study. Crit Care. 2005;9(6):R764-70. • Moore, L. J., et al. Validation of a Screening Tool for the Early Identification of Sepsis. J Trauma. 2009;66: 1539-1547. • Nguyen, H. B., et al. Implementation of a bundle of quality indicators for the early management of severe sepsis and septic shock is associated with decreased mortality. Crit care med. 2007 Apr;35(4):1105-12. • Rivera, C. Every minute counts. Nurs2008 Crit care. 2008;3(2):42-50. • 6. Zubrow, M. T., et al. Improving care of the sepsis patient. J Com J Qual Pat Saf 2008;34(4):187-91.