Download
1 / 81
820 likes | 1.15k Vues
GONADAL DRUGS. Ma. Janetth B. Serrano, M.D., DPBA. Gonads: Ovary. Quiescent during rapid growth & maturation At puberty: - Gonadarche → beginning of ovarian function - Menstrual cycle → a 30- to 40- year period of cyclic function → manifested as regular episodes of bleeding

E N D
GONADAL DRUGS Ma. Janetth B. Serrano, M.D., DPBA
Gonads: Ovary • Quiescent during rapid growth & maturation • At puberty: - Gonadarche→ beginning of ovarian function - Menstrual cycle → a 30- to 40- year period of cyclic function → manifested as regular episodes of bleeding - Menopause → if ovaries fail to respond to gonadotropins secreted by the ant. pituitary.
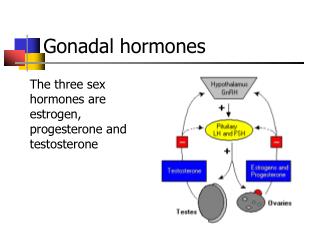
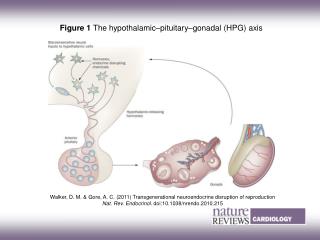
Gonads: Ovary Hypothalamus↓ GnRH ↓ Anterior Pituitary↓ FSH / LH↓ Ovary / Testes Estrogen/ Testosterone/ Progestins Androgens NEUROENDOCRINE CONTROL OF THE MENSTRUAL CYCLE (-) (-)
Gonads: Ovary • DISTURBANCES IN OVARIAN FUNCTION: • environmental or emotional stress • anovulatory cycles: • eating disorders (bulimia,anorexia) • severe exercise • organic causes: • pituitary prolactinomas • ovary gives rise to: • androgen producing neoplasms (arrhenoblastoma, Leydig cell tumors, estrogen producing granulosa cell tumors) • minor causes: inflammatory or neoplastic processes that inluence function of the ovaries, uterus or pituitary
Estrogens • Naturally occuring: • 17β – estradiol (most potent) • Estrone • Estriol
Estrogens • Immediate precursors: Androstenedione / Testosterone • Ovaries – principal source of circulating estrogen • Other sources: • liver (estrone, estriol fr. estrsdiol) • Peripheral tissues (fr. androstenedione & other androgens) • Pregnancy: fetoplacental unit ( fetal adrenal zone, secreting androgen precursor, placenta) • Stallion – equilenin and equilin • Soybeans - flavinoids
Estrogens PHARMACOKINETICS • binds strongly to SHBG and less to albumin • estrdiol converted by the liver to: • estrone & estriol • 2-hydroxylated derivatives • conjugated metabolites catechol estrogens • may serve as neurotransmitters in the CNS • converted by COM-T to 2- and 4- methoxy compounds • excreted in the bile; small amounts in breastmilk
Biosynthetic Pathway for Estrogens: Dehydroepi- 16 α-OHase 16α-Hydroxyde- 16α-Hydroxydehy - androsterone hydroepiandros hydroepiandros- terone terone Androstenedione aromatase Estrone Estriol TESTOSTERONE aromatase ESTRADIOL
Estrogens MECHANISM OF ACTION • primarily by regulating gene expression • SHBG-bound estrogens dissociate & enter cell bind to their receptor • Receptor-hormone complex bind to Estrogen Response Elements or ERE’s (specific sequence of nucleotides)
Estrogens PHYSIOLOGIC EFFECTS 1. Female maturation • required for 2 O sexual characteristics: • stimulate development of vagina, uterus & tubes • breast development stromal development, ductal growth and accretion of fat • accelerated growth phase and closure of epiphysis • axillary and pubic hair • regional pigmentation of axilla, areola & genital area
Estrogens PHYSIOLOGIC EFFECTS 2. Endometrial effects • hyperplasia of the endometrium continuous exposure 3. Metabolic and Cardiovascular effects: • Lipoprotein: HDL , slight LDL • plasma cholesterol • plasma triglycerides 4. Blood Coagulation • enhance coagulability • Factors II, Vii, IX, X • antithrombin III • plasminogen level platelet adhesiveness
Estrogens CLINICAL USES • Primary hypogonadism • associated with hypopituitarism • Turner’s syndrome – ovarian dysgenesis with dwarfism • treatment begins at puberty – 11 to 13 years: • to stimulate development of 2O sexual characteristics and menses • to prevent osteoporosis • to avoid physiologic consequenses of delayed puberty and estrogen deficiency • Dosage: Conjugated estrogen 0.3 mg or Ethinyl estradiol 5-10ug • on days 1 to 21 of each month • when growth is completed Chronic Tp with estrogen and progestins
Estrogens CLINICAL USES 2. Postmenopausal Hormone Replacement Therapy • major indication • prevent bone loss (osteoporosis) • decrease vasomotor symptoms • prevention of cardiovascular disease • prevent vaginitis • Dosage: Conjugated Estrogen – 0.3 to 1.25 ug/day Ethinyl Estradiol – 0.01 to 0.02 mg/day
Estrogens CLINICAL USES • Replacement Regimen: A: Sequential hormone administration 1. Estrogen for first 25 days 2. MPA (Medroxyprogesterone acetate) 10 mg/day for the last 10 to 14 days of estrogen therapy 3. No hormone treatment for 5 to 6 days (+) withdrawal bleeding B: “Continuous” hormone administration 1. estrogen 0.625 mg given continuously on a daily basis 2. progestin MPA 2.5 to 5 mg jointly given during the first 10 to 13 days of each month 3. no cyclic bleeding • PROGESTINS – included to decrease endometrial hyperplasia and incidence of endometrial carcinoma
Estrogens CLINICAL USES 3. Contraception • major indication 4. OTHER USES: • DUB & intractable dysmenorrhea (Es + Progestins) • Hirsutism & amenorrhea • DES prostate carcinoma • Severe cystic acne
Estrogens ADVERSE EFFECTS • postmenopausal bleeding • carcinogenic action – breast, endometrial • thromboembolic disease, HPN • GB disease, cholestasis • Nausea & breast tenderness • Migraines • Changes in mood
Estrogens CONTRAINDICATIONS • CONTRAINDICATIONS: • estrogen- dependent neoplasms • undiagnosed genital bleeding • history of liver disease • history of thromboembolic disorder • heavy smokers
Gonadal Inhibitors Anti - Estrogens ANTI-ESTROGENS: A. Tamoxifen • a competetive partial agonist inhibitor of estradiol at estrogen receptors • nonsteroidal agent given orally • initial half-life: 7 to 14 hours • excretion: liver • Cl. Indication: palliative/adjuvant tp of breast CA • Dosage: 10-20 mg BID orally • Adverse effects: nausea & vomiting • hot flashes • vaginal bleeding, menstrual irregularities, skin rash • risk of endometrial cancer • loss of lumbar spine bone density • plasma lipid changes risk of atherosclerosis
Gonadal Inhibitors Anti - Estrogens B. TOREMIFENE C. RALOXIFENE • “selective estrogen receptor modulator” • high first pass effect, large Vd • long half-life: >24 hours • Cl. Indication: prevention of postmenopausal osteoporosis D. CLOMIPHENE • competetive inhibitor of endogenous estrogen • partial agonist at pituitary • ovulation-inducing agent
Gonadal Inhibitors Anti - Estrogens ESTROGEN SYNTHESIS INHIBITORS 1. GnRH • continuous administration prevents ovarian synthesis of estrogen 2. AMINOGLUTETHIMIDE • inhibits aromatase activity 3. AROMATASE INHIBITORS a. Testolactone – weak inhibitor b. Anastrozole • selective nonsteroidal inhibitor of aromatase • effective in tamoxifen-resistant breast tumors c. Letrozole – similar to anastrozole d. Exemestane • steroid molecule that irreversibly inhibits aromatase • advanced breast CA e. Fadrozole – newer oral nonsteroidal
Ovulation Inducing Agents CLOMIPHENE • Partial agonist at estrogen receptors • MOA: secretion of gonadotropins & estrogens by inhibiting estradiol’s negative feedback effect • Effects: 1. stimulate ovulation in females with amenorrhea & other ovulatory disorders 2. blocks inhibitory influence of estrogen on the hypothalamus • Clinical Use: 1. Treatment of disorders of ovulation in patients wishing to be pregnant • no use in ovarian & pituitary failure • single ovulation induced by a single course of therapy
Ovulation Inducing Agents CLOMIPHENE • Dosage: 50 mg/ d X 5 days • (+) ovulation same course repeated until pregnancy occurs • (-) ovulation 100 mg/d X 5 days if (+) menses & ovulation, start next course on 5th day of cycle • Adverse Effects: • hot flushes – most common • eye symptoms – due to intensification & prolongation of after images • ovarian enlargement • multiple pregnancy – 10% • rare: headache, constipation, allergic reactions, reversible hair loss • C/I: patients with enlarged ovaries • > 1 year tx: assted with low-grade ovarian CA
Progestins • Natural: PROGESTERONE • most important progestin in humans • precursor to estrogens, androgens, adrenocortical steroids • synthesized in the ovary (corpus luteum), testis, adrenals, placenta
Progestins • Synthetic: A. 21-Carbon compounds (Progestrone & derivatives) • Hydroxyprogesterone - longest DOA (8-14 days) • Medroxyprogesterone • Megestrol B. 17-Ethinyl testosterone derivatives • Dimethisterone
Progestins C. 19-Nortestosterone derivatives (3rd generation) 1. Desogestrel 6. Norethindrone acetate 2. Norethynodrel 7. Ethynodiol acetate 3. Lynestrenol 8. L-Norgestrel 4. Norethindrone 9. Gestodene 5. Norgestimate • MECHANISM: • binds to progesterone receptors
Progestins PHYSIOLOGIC EFFECTS • Carbohydrate metabolism • insulin levels • insulin response to glucose • promote glycogen storage in the liver • favor fat deposition • promote ketogenesis • compete with aldosterone • ( Na+ reabsorption)
Progestins PHYSIOLOGIC EFFECTS • body temperature • ventilatory response to CO2 • depressant & hypnotic effects • Sexual characteristics: • breast: alveolobular devt. of the secretory apparatus • endometrium: maturation & secretory changes • Important in the maintenance of pregnancy • plasma amino acid levels urinary nitrogen excretion
Progestins Synthetic progestins: • no androgenic activity: • desogestrel, • norgestimate, • gestodene
Progestins PHARMACOKINETICS • rapidly absorbed • approx. half life: 5 min • stored in body fats • metabolite: Pregnanediol • Elimination: urine as Pregnanediol glucoronate
Progestins CLINICAL USES • Hormone replacement therapy • Hormonal contraception • Ovarian suppression: > dysmenorrhea > hirsutism • endometriosis > uterine bleeding • Premenstrual syndrome • progesterone & MPAProgestins
Progestins CLINICAL USES • Diagnostic test Estrogen secretion • Progesterone 150 mg/d or MPA 10 mg/d for 5-7 days withdrawal bleeding in amenorrheic patients • Single drug: • MPA 150 mg IM every 90 days prolonged anovulation and amenorrhea • MPA 10-20 mg p.o. twice weekly or 100 mg/m2 I.M. every 1-2 weeks prevent menstruation
Progestins ADVERSE EFFECTS • BP • HDL androgenic progestins
Other Ovarian Hormones 1. ANDROGENS • testosterone, androstenedione, dehydroepiandrosterone • responsible for hair growth, stimulation of libido, metabolic effects • asstd. with hirsutism & amenorrhea 2. INHIBIN and ACTIVIN • dimer (inhibin) inhibits FSH secretion • dimer (activin) FSH secretion
Other Ovarian Hormones 3. RELAXIN • found in the ovary, placenta, uterus • glycogen storage and water uptake • facilitates dilatation & shortens labor 4. Non steroidal substances • corticotropin-releasing hormone, follistatin, PG • with paracrine effects within the ovary
Gonadal Inhibitors Anti - Progestins 1. MIFEPRISTONE (RU486) • a derivative of ‘19-nor progestin norethindrone’ • a potent competetive antagonist of progesterone and glucocorticoid at their receptors • acts as partial agonist if progestin is absent • (+) luteolytic in women at midluteal period • Pharmacokinetics: • oral route with good bioavailability • plasma half-life: 20 to 40 hours • hepatic metabolism • elimination: feces
Gonadal Inhibitors Anti - Progestins MIFEPRISTONE • Therapeutic indications: 1. Medical abortion during the first trimester • dosage: 400-600mg/day X 4 days or 800 mg/day X 2 days + Prostaglandin 48 hrs after antiprogestin to myometrial contraction & ensure expulsion of detached blastocyst • major adverse effect: prolonged bleeding • combination: 600 mg o.d. SD + PG E1 vaginal pessary or 1 gm. Misoprostol (95% effective during 1st 7 weeks post conception) • adverse effects: vomiting, diarrhea, abdominal pain, pelvic pain
Gonadal Inhibitors Anti - Progestins MIFEPRISTONE Therapeutic indications: 2. Postcoital contraceptive • prevents implantation • dosage: 600 mg SD 3. Induction of labor after fetal death & at the end of 3rd trimester 4. Tx of endometriosis, leiomyoma, breast cancer, meningiomas
Gonadal Inhibitors Anti - Progestins DANAZOL • an isoxazole derivative of ethisterone • weak agonist at progestational, androgenic and glucocorticoid receptors • inhibitor of gonadal function • MOA: binds to receptors initiate androgen-specific RNA synthesis • Major metabnolite: ETHISTERONE –with progestational & androgenic effects • t ½ = >15 hrs • Elimination: urine & feces
Gonadal Inhibitors Anti - Progestins DANAZOL Clinical Uses: • treatment of endometriosis • 600 mg/d reduced to 400 mg/d after 1 mo. then 200 mg/d after 2 mos (85% with improvement in 3-12 mos) • fibrocystic disease of the breast • hematologic or allergic disorders: • hemophilia, Christmas disease, ITP, angioneurotic edema
Gonadal Inhibitors Anti - Progestins DANAZOL Major adverse effects: • weight gain, edema, breast size, acne & oily skin, hair growth, headache, deepening of voice, hot flushes, muscle cramps • Caution: hepatocellular damage • C/I: pregnancy & lactation urogenital abnormalities
Gonads: Testis • both gametogenic & endocrine functions • Anterior Pituitary FSH (+) (-) (-) LH TESTOSTERONE Activin Inhibin Sertoli cells Mullerian Inhibitory factor ESTRADIOL LEYDIG CELLS SEMINIFEROUS TUBULES
Testosterone TESTOSTERONE • most important androgen secreted by the testes • 8 mg/day produced daily • 95% by Leydig cells; 5% by androgens • Plasma levels: • 0.6 ug/dL after puberty • (declines after 50 years of age) • 0.03 ug/dL = females
Gonads: Testis HYPOTHALAMUS GnRH Anterior Pituitary LH Testes Ketoconazole Spirinolactone TESTOSTERONE 5α - Reductase FINASTERIDE Dihydrotestosterone Androgen Receptor Complex Flutamide Cyproterone Spirinolactone Androgen Response Element Expression of Appropriate genes in androgen-responsive cells
Gonads: Testis Other androgens/hormones produced: • dihydrotestosterone • androstenedione • dehydroepiandrosterone • pregnenolone • progesterone & 17-hydroxylated derivatives
Testosterone • BINDING: 65% - SHBG 2% - free 33% - albumin • METABOLISM: Testosterone converted to dihydrotestosterone (major active androgen) by 5--reductase
Testosterone PHYSIOLOGIC EFFECTS: A. Changes during puberty(Adrenarche) • testosterone & 5 dihydrotestosterone penile & scrotal growth • skin pubic, axillary & beard hair (Androstenedione, DHEA) more active sebaceous glands thicker & oilier skin • larynx vocal cords thicker low pitch voice • skeletal growth
Testosterone PHYSIOLOGIC EFFECTS: B. increase lean body mass C. male development (2O sexual characteristics) • stimulate development & maturation of sperm • stimulate development of the epididymis, vas deferens, seminal vesicles, scrotum, penis, prostate D. anabolic effect on muscle & bone mass • increase protein synthesis, decrease protein breakdown • measured by urine nitrogen secretion
Testosterone PHYSIOLOGIC CHANGES E. musculinization in females F. metabolic effects: • hormone binding • liver synthesis of clotting factors, triglyceride, lipase, anti-trypsin • HDL • stimulate renal erythropoietin secretion
Testosterone PREPARATIONS: Natural androgen:testosterone Synthetic: Parenteral: ~ testosterone proprionate ~ testosterone enanthate ~ testosterone cypionate Oral: ~ Danazol ~ Fluoxymesterone ~ Methyltestosterone Anabolic steroids: ~ Oxandrolone ~ Stanozolol
Testosterone CLINICAL USES: 1. Androgen replacement therapy in men • hypogonadism • pituitary deficiency • given at puberty growth spurt & 2O sexual characteristics • Dosage: Testosterone enanthrate • 50 mg IM q 4 wks; then q 3 wks; then q 2 wks (@ change at 3 mos interval) • double dosage at 100 mg q 2 wks until maturation is complete then adult dose of 200 mg q 2 wks