Download
1 / 31
341 likes | 436 Vues
Understand pediatric stroke incidence, presentation, causes, and barriers to care, along with management strategies. Learn about focal and nonlocalizing manifestations, perinatal stroke, childhood stroke, and case studies.

E N D
Pediatric stroke Sarah Cobb,MD Assistant Professor Child Neurology Arkansas Children’s Hospital
Pediatric Strokes: up to 25/100,000 (combined acute ischemic and hemorrhagic) • As common as pediatric brain tumors. • Mortality rate 2-11% • Neuro deficits up to 75% • Only 2% receive tPA • Incidence is likely increasing due to: • Increased awareness • Better imaging • Increased survival in previously lethal diseases that predispose to stroke (CHD, leukemia, SCD)
Males are more likely to have any type of stroke when compared to females (hemorrhagic or ischemic) • 16.8 vs 11.8 • African American children 2x more likely to have stroke (independent of SCD). • Hispanic children seem to be the at lowest risk.
Perinatal stroke: occurring from 28 weeks gestation until 28 post-natal days of life. • Childhood stroke: occurring from 28 days to 18 years
Perinatal stroke: • Arterial ischemic infarction accounts for ~80% strokes in perinatal strokes. • Ischemic stroke occurs in about 1 in 3500 newborns. • Almost 6 times greater incidence than in older children. • Childhood stroke
Perinatal stroke • Presentation: • >90% present with seizures. • Causes: • High maternal coagulation factors (to protect mom during delivery) • Break down of placenta--> clots to baby • cardiac lesions, coagulation disorders, infection, trauma, and asphyxia • Almost never find a single definite etiology • Evaluation: • MRI/MRA • Hypercoaguable workup is not indicated. • Management: • Supportive care: controlling seizures, the optimization of oxygenation, and the correction of dehydration and anemia.Antiplatelet therapy such as aspirin and anticoagulation is rarely indicated • Hyperacute stroke therapies (thrombolytics and mechanical thrombectomy) are rarely considered in neonates with AIS because there is no evidence for their use.
Focal neurologic manifestations- • Hemiparesis and hemifacial weakness in 67 to 90 percent • Speech or language disturbance in 20 to 50 percent • Visual disturbance in 10 to 15 percent • Ataxia in 8 to 10 percent • Nonlocalizingmanifestations- The most frequent nonlocalizing manifestations in arterial ischemic stroke are the following: • •Headache in 20 to 50 percent • •Altered mental status in 17 to 38 percent • •Vomiting in approximately 10 percent • Seizures – Seizures at stroke onset occur in 15 to 25 percent of children with arterial ischemic stroke; the frequency is highest in younger children, particularly those less than six years of age
Hemorrhagic stroke • Nontraumatic, spontaneous ICH, IVH, and SAH in childhood are caused by structural lesions in up to ≈75% of cases, with brain AVMs found most commonly
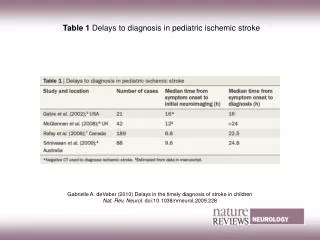
Barriers to care in pediatric stroke • Delay in diagnosis- • Parents may not recognize or consider stroke in their child. • Many physicians may not consider stroke in the differential of children, especially if they present to an outside hospital first. • One study reported a median time from symptom onset to radiographic confirmation of 15-24 hours. • In one retrospective study, the average time from onset of symptoms until diagnosis was 35.7 hours. • Children may present differently than adults. • Children may present with first time seizure with post-ictal neuro deficits (up to 30% of kids will present with seizure vs 5% of adults) • Irritability • Use of non-dominant hand • Refusal to walk • Limited access to imaging for children. • Harder to get MRI since anesthesia may be needed for younger children. • Very limited clinical guidelines and systematic research. NO randomized clinical trials for intervention.
Case 1: • 3-year-old Caucasian boy acutely developed right arm and leg weakness, right facial droop and stopped talking while playing with dad around 18:30. • Presented to an outside ER within the hour. • Per outside ER records: “child arrives with drooling. Does not move R arm or leg. Child does not respond verbally. R facial droop noted.” • ER concerned for ingestion. Gave Narcan (no improvement). Toxicology screen was negative. • Transferred to ACH. In our MRI around 23:30.
Left basal ganglia stroke -Has very mild residual right hand weakness. -Extensive workup did not reveal a cause of his stroke. -No recurrent episodes on aspirin 81 mg.
Case 2 • 17 year old girl with a history of migraines presented to local hospital with acute onset expressive aphasia and headache. • Was found to be very hypertensive. Her blood pressure and headache were treated and she was discharged from the ED with no improvement in her aphasia. • Due to persistent aphasia (>24 hours) she presented to our ED the following day. Brain MRI was done which showed a left middle cerebral artery infarct as well as multiple areas of encephalomalacia.
Causes • Cardiac: #1 cause of AIS in children. Accounts for up to 1/3 of AIS in children. • Hematologic: • Infectious:
Since Aug 2015, we had 96 stroke activations and 15 (~15%) were confirmed strokes. • Stroke mimickers are much more common in children • Hemiplegic migraine • Todd’s paralysis • Hypoglycemia • Encephalitis • Tumor • Ingestion
Risk factors • Sickle cell disease • CHD • Prothrombotic state • Recent head and neck infections • Recent viral illness • Dehydration • Autoimmune disorder • Arteriopathies • About 25% are considered “idiopathic”
IR will review the images. If there is a large vessel stroke and IR feels that intervention is warranted, then patient will transfer to UAMS to have the procedure done (protocol to make that happen smoothly is in the works). Afterward, will return to ACH PICU.
Acute treatment • Thrombolysis: Alteplase (tPA) is not FDA approved in children <18 years of age. There are case reports, national registry data from the US and international registry data of IV or intraarterial thrombolysis use in small numbers of children. • Effectiveness, safety and dose has not been established • About 2% of children with AIS are treated with tPA.
alteplase • Recombinant tissue-type plasminogen activator • Converts plasminogen to plasmin which facilitates clot breakdown • Children have immature fibrinolytic system • Low baseline free-tPA • Plasminogen activator inhibitor-1 (inhibitor of tPA) increased Recommended dose: total dose 0.9 mg/kg (max 90 mg), 10% IV bolus over 5 minutes, remainder over 55 minutes
Thrombolysis in Pediatric Stroke (TIPS): multicenter prospective treatment study from 2010 to 2013 to determine safety dosing and feasibility of IV tPA in children ages 2-17 years. -3 dosing tiers (0.75, 0.9, 1 mg/kg) 93 children screened • 43/93 (46%) had an acute ischemic stroke. • 21 had contraindications to tPA. • 10 presented outside of treatment window • 2 lacked evidence of arterial occlusion on imaging • 9 excluded for low Peds NIHSS score (<6) • ONE patient met criteria for tPA. NIH closed the study in 2013 for lack of enrollment.
Helped create a standardization of care for pediatric stroke. • Many hospitals have designed their stroke and tPA protocols after the TIPS study tPA candidates: -24 months or older -last seen well <4.5 hours from presentation -confirmed clot on neuroimaging -PedsNIHSS >4 (some use 6)
Acute treatment • Thrombectomy: No studies looking at mechanical thrombectomy in children but can be considered on individual basis for some patients <18 years with a documented large vessel occlusion and AIS.
Supportive care • All patients with confirmed stroke will initially go to PICU. • Close observation during first 48-72 hours after stroke to monitor for changes in neuro exam, physiologic derangement, signs of increased ICP, recurrent stroke, etc.
Supportive care • Head of bed should be flat for at least 24 hours to increase perfusion. Can exacerbate edema but would be unlikely to have significant swelling in first 24 hours. If concerned for increased ICP then HOB at 30 degrees. • NPO until evaluated for safe eating • Euvolemia • Normoglycemia (glucose 60-200) • Prevention of hyperthermia is very important and should use acetaminophen liberally. • HTN management • Treat seizure aggressively if they occur
Work up • Hypercoagulable labs • ECHO with bubble study • Swallow study
Secondary prevention • As with acute treatment, there are no controlled trials or studies examining the effectiveness of specific treatment for secondary prevention in children. • Antiplatelet therapy is mainstay for secondary ischemic stroke prevention. Once dissection and cardioembolic causes are excluded, the American College of Chest Physicians guidelines for antithrombotic therapy in children suggest daily aspirin for a minimum of 2 years. • Arterial dissection: ACCP recommends LMWh or warfarin for at least 6 weeks. AHA recommends 3-6 months.
prognosis • A study of national registry data from the US reported that in hospital mortality after AIS was 4.7 percent. Similarly, among 612 children with AIS in an international database, the mortality rate prior to hospital discharge was 3%. • Despite neural plasticity, 60-75% of children will have some degree of persistent disability. • Epilepsy is a long-term risk. 13% by 5 years and 30% by 10 years after a childhood stroke.