Download
1 / 48
510 likes | 749 Vues
Strategies for Managing Disruptive Behavior and Conflict. Nicola Schiebel MD, FRCPC Consultant-Emergency Medicine Carol Fahje MS, RN, BC Nursing Education Specialist Emergency Department. Objectives. Review cultural/human factor issues that affect our day to day interactions

E N D
Strategies for Managing Disruptive Behavior and Conflict Nicola Schiebel MD, FRCPCConsultant-Emergency Medicine Carol Fahje MS, RN, BC Nursing Education Specialist Emergency Department
Objectives Review cultural/human factor issues that affect our day to day interactions Types of conflict Examples of how bad behavior harms patients Abusive and Disruptive behavior Designing a system to address culture change Creating Psychological Safety Discuss training and tools for managing conflict Effective reinforcement and feedback
Sources of Conflict What to do? (task related) Whose job is it? (team process) Interpersonal differences Bullying/abusive behavior
Abusive Behavior Should we care??
2007 Headlines “Rhode Island Hospital Reprimanded for Wrong Site Surgeries” Posted by Jane Akre Tuesday, November 27, 2007 4:36 PM EST • 3 events in 6 years involving same OR
Universal Protocol Fails “Nurses may be afraid to speak up” The mistakes at Rhode Island Hospital suggest that the precautions can still be thwarted by the human element: • Ego and overconfidence on part of surgeons; • Timidity on the part of the nurses too afraid to speak up when they see something wrong
Where does a culture of intimidation lead? “Wrong-Site Surgery: Hospital Ordered to Install Video Cameras in OR” Nov. 2, 2009; MSN news Hospital fined $150,000 in wrong-site surgery Rhode Island Hospital has had five such incidents since 2007
Increase in Medical Errors due to Human Factors Perceptions Memory Decision-making Ability to do tasks Attitudes • Mutual Trust • Psychological Safety Team terrified to speak up • Performance • Safety • Accuracy Staff bullied into not following SOP
Impairs Decision Making • S- 67 yo male tachycardia, SOB and hematemesis / melena • B- 3 days post thoracic surgery for lung mass; • PMHx CAD; on high dose B-blocker • HR 130, BP 100/70, T- 37, RR 22, SaO2=99% • RN is scared to call MD (bully); report is poor as she is very nervous; does not get a chance to tell him about bleeding, only vomiting. • MD interrupts, assumes tachycardia due to missed B-blocker; orders B-blocker and hangs up.
Impairs Decision Making • RN calls Rapid Response Team (RRT) and waits to give medication • Team arrives and just starts to get history when MD arrives. • Observe how behavior results in rushed decision making, and inappropriate medication administration.
Psychological Safety • Critical to Team Performance • People need to feel safe to speak up: • Does it feel safe to speak up? • Will I be treated with respect? • Will it help fix the problem? • If you don’t get the right answers, then it gets risky
Impact of Disruptive Behaviors Source: Rosenstein AH, O'Daniel M. A survey of the impact of disruptive behaviors and communication defects on patient safety. Jt Comm J Qual Patient Saf. 2008:34;464-471.
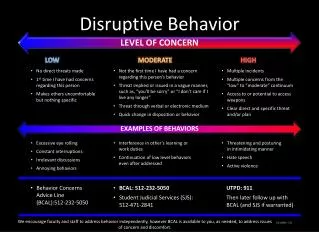
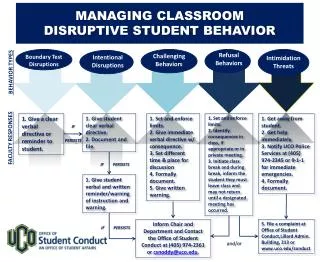
What is considered unacceptable? • Any disruptive behavior which either overtly or covertly compromises safe and quality patient care. • Verbal outbursts • Physical outbursts • Uncooperative attitudes • Condescending voice or tone intonations The Joint Commission Sentinel Event Alert Issue 40, July 9, 2008
How do you change it? • Create policies which specifically identify expectations • Assess current culture and develop educational plan to address deficiencies • Embed in all levels of the institution • Job descriptions • Competencies • Acknowledgements
Mutual Respect • Define the Purpose of the Policy • What is the expectation of staff? • Example: Mutual respect is expected of every member of the staff. • What are the rights of the employees? • Example: Freedom from disruptive and/or behavior and harassment are rights of every employee.
Mutual Respect: Create Specific Policy Statements • Determine the action that staff should take who have experienced disrespectful behavior. • Example: Employees should report their experience to their supervisor, administrator or human resources as soon as possible after the event. • Determine the action the supervisors are required to do when report such incidents • Example: The Supervisor should listen and document the incident. The report should be forwarded to _____. The hospital will investigate complaints and take appropriate corrective action. The privacy of the employee making the complaint will remain confidential.
Mutual Respect: Policy Statements Continued • Determine ramifications for abuse. • Example: Retaliation will not be tolerated and may result in _____________.
Disruptive Behavior • Define the Purpose of the Policy • Example: This policy will define expectations for acceptable conduct of staff members.
Disruptive Behavior: Create Specific Policy Statements • Define expectations for conduct: • Example: Staff members are to conduct themselves in a cooperative and professional manner at all times. Professional standards dictate that interactions are conducted with mutual respect and courtesy. • Define how disruptive behavior reflects on the person and the institution: • Examples: Safe patient care and quality may be compromised when professional standards of communication are violated. This reflects poorly on both the individual and the institution.
Disruptive Behavior: Policy Statements Continued • Determine ramifications of what would occur as a result of repeated proven disruptive behavior/communication. • Letter of warning? • Administrative Leave? • Termination? • It is up to your institution to determine the ramifications.
Example of Job Description Essential Functions • Fosters mutual respect among all team members • Treats others with dignity and contributes to a work place free from harassment and disrespectful behavior
Training • All current staff need to demonstrate knowledge and behaviors as defined in policy • Annual performance reviews • Competencies • Incorporate expectations into new staff orientation • Leadership/Management need to know what their responsibilities are when made aware of disrespectful behavior
Competencies • FOSTERING MUTUAL RESPECT/DIVERSITY – creates an atmosphere of respect, appreciates individual differences and addresses disrespectful behavior appropriately • Acknowledges and respects differences among colleagues and patients • Appreciates ideas, values, and talents of others; and leverages resources appropriately • Confronts disrespectful/inappropriate behavior among all colleagues
Tools and Strategies for Managing Conflict and Disruptive Behavior
Advocacy and Assertion • Advocate for the patient • Invoked when team members’ viewpoints don’t coincide with that of a decision maker • Assert a corrective action in a firm and respectfulmanner
The Assertive Statement • Respect and support authority • Clearly assert concerns and suggestions • Use an assertive statement (nonthreatening and ensures that critical information is addressed) • Make an opening • State the concern • Offer a solution • Reach an agreement
Example of Advocacy/Assertion • Dr. Schiebel I am concerned. • Mr. Smith’s saturations are dropping whenever he coughs and fights ventilator. His BP is falling with the sedation and it is not helping the cough. • I really feel he needs neuromuscular blockade so he can maintain oxygenation. • Can I get an order to give him some vecuronium?
Critical Language • Key phrases understood by all to mean “stop and listen to me – we have a potential problem” • United Airlines CUS Program – “I’m concerned…I’m uncomfortable…this is unsafe – I’m scared.” • Allina – “I need some clarity” - Dr. M. Leonard
Two-Challenge Rule Invoked when an initial assertion is ignored… • It is your responsibility to assertively voice yourconcern at least two times to ensure thatit has been heard • The member being challenged must acknowledge • If the outcome is still not acceptable • Take a stronger course of action • Use supervisor or chain of command
Another Example of Critical Language “I need some clarity.”
SBAR for critical communication • S- 67 yo male tachycardia, SOB and hematemesis / melena • B- 3 days post thoracic surgery for lung mass; PMHx CAD • HR 130, BP 100/70, T- 37, RR 22, SaO2=99% • A – The surgery fellow wanted to give metoprolol since he missed his dose, but I was not comfortable with this because I think he is bleeding and this is causing his HR=130. • R – Could you assess patient and see what you think?
Culture Change Comes Last, Not First! • New approaches sink in after success has been proven • Feedback and reinforcement are crucial to buy-in • Individuals in leadership positions need to be on board • Otherwise, the old culture will reassert itself
Psychology of Change • Organizations that measure and reinforce desired behaviors consistently observe those behaviors in day to day practice. • Work is task based and processes for workers to complete their tasks need to be understandable and understood. • People do not change, BUT you can change their behaviors by changing the environment in which they work. Eduardo Salas
Video or Tape Review Conferences • Focus on Behaviors • Dramatic changes in behavior possible if done well
Build culture of teams • Rapid Response Systems • Designs training of medical and nursing students to include teamwork training • Provide high quality feedback and opportunities to practice
What Is Feedback? “Feedback is the giving, seeking, and receiving of performance-related information among the members of a team.” (Dickinson and McIntyre 1997)
Characteristics of Effective Feedback Good Feedback is— • TIMELY • RESPECTFUL • SPECIFIC • DIRECTED toward improvement • Helps prevent the same problem from occurring in the future • CONSIDERATE
Acknowledge it! Example of highly esteemed award given at Mayo Clinic. Note first qualification on the list. • Individual Award for Excellence • Mutual respect ( kindness, courtesy, respect and dignity.) • Commitment to Quality as it relates to continuous improvement and process change. • Positive Work Atmosphere (teamwork, integrity, trust) • Commitment to Service Excellence.
Change • Will it be worth it? • Can I do it?