Carotid Artery Stenting in Asymptomatics
Carotid Artery Stenting in Asymptomatics. Oscar A. Mendiz. MD.FACC.FSCAI Chief Interventional Cardiology SOLACI President. August 2012. Conflictos de Interes. Nombre: Oscar A. Mendiz Medtronic : Proctor para CoreValve. Elli Lilly ; Speacker AstraZeneca : Advisory Board


Carotid Artery Stenting in Asymptomatics
E N D
Presentation Transcript
Carotid Artery Stenting in Asymptomatics Oscar A. Mendiz. MD.FACC.FSCAI Chief Interventional Cardiology SOLACI President August 2012
Conflictos de Interes • Nombre: Oscar A. Mendiz • Medtronic: Proctor para CoreValve. • Elli Lilly; Speacker • AstraZeneca: Advisory Board • Sponsors para viajes a Congresos: Acher (Cook), Angiocor (AGA), Cordis, BSCI, Cordis, Medikar, Sanofi. 2
Carotid Artery Disease Carotid Stenosis Symptomatic: ~25% Asymptomatic: ~75% Normal Risk High Risk Normal Risk High Risk ~15% ~10% ~50% ~25% Modified from M Jaff, 2007
Historical use only?NASCET Trial: events at 5 years in asymptomatic patients Although some data suggests you cannot use “>80%” as lone criteria in asymptomatic pts, it is somehow arbitrary Only 15% were receiving lipid lowering agents!!!! • Note: • 1-45% of the neuro events were NOT related to the carotid lesion • 2-Similar events in >60 and >70% stenosis Barnett HJM, et al. JAMA. 2000;283:1429-1436
0.5 1.0 2.0 Medical Treatment Improvements ACE- Inhibitors vs. Placebo Cardiovascular Endpoints Number of Events/ Total Patients Relative Risk (95% CI) ACE-I Placebo 0.70 (0.57-0.85) 0.80 (0.72-0.89) 0.84 (0.68-1.04) 0.74 (0.64-0.85) 0.84 (0.76-0.94) Stroke 166/6060 240/6064 CAD 539/6060 672/6064 CHF 154/6060 183/6064 CV death 307/6060 416/6064 Total death 533/6060 632/6064 Blood Pressure Lowering Treatment Trialists’ Collaboration Lancet, 2000; 355: 1955-64; HOPE, PART2; QUIET, SCAT
Medical Treatment Improvements Statins: Stroke Reduction in High Risk Ptes Mark C Bates. www.tctmd.com
Medical Treatment Improvements: Statins Carotid Intima Media Thickness reduction with Atorvastatin Improvements on TCD Outcomes 471 Patients with ACS Received Mxm after 2003 272 pts Received Mx before 2003 199 pts HITS on TCD 12.6% HITS on TCD 3.7% Conclusion: With more intensive Mx, regression of carotid plaque occurs in half our patients; this has resulted in a marked decline of TCD microemboli and clinical events among patients with ACS”. Conclusion: ‘Marked LDL reduction (<100 mg/dl) with high potency statins results in regression at 1 year’ J. David Spence,et al..More Intensive Medical Therapy has Reduced Microemboli and Cardiovascular Eventsin Patients with Asymptomatic Carotid Stenosis Abstract presented AHA San Diego 2009 Taylor AJ et al. Circulation 2002; 106: 2055-2060 Mark C Bates. www.tctmd.com
Annual TIA & Stroke rate reduction in asymptomatic control arms of randomized trials
Caveats: 1. Different patient population (“low risk”) 2. Improved outcomes with medical therapy have been under the microscope of a clinical trial driven strict follow-up. Patients are selected based on their willingness to comply with these strict guidelines and investigators are admonished for failing to monitor compliance Ann L. Abbott. Stroke. published on-line Aug 20,2009 Mark C Bates. www.tctmd.com
Improvements on CAS Outcomes over the time Cremonesi Alberto. Linc 2012
Improvements on CAS Outcomes over the time: Post Market registries Note: Major Stokes only 0.9% Gray W et al. Circ Cardiovasc Intervent 2009, 2: 159-166 March Mark C Bates. www.tctmd.com
30-day Composite Endpoint in US Carotid Stenting Registries
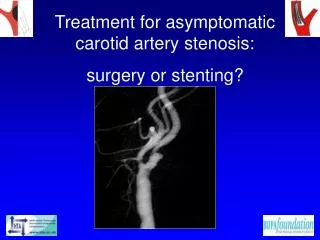
Asymptomatic Carotid Artery Stenosis CEA Best Mx
What do we know about Surgery?: Carotid Endarterectomy Surgery for Carotid Stenosis NASCET Collaborators. N Engl J Med 1994;325:445-453. ACAS. J Am Med Assoc 1995;273:1421-1428. 12
ACAS Study: CEA Not Effective in Women Stroke and Death @ 5 Years 14 12 10 8 Percent 6 4 2 0 Med CEA Med CEA Men Women Rothwel PM; et al. Lancet 2004:364:1122-3
Revascularization for Asymptomatic Carotid Artery Stenosis • Background: • Approximately 20% of strokes are attributable to carotid stenosis. • However, the number of asymptomatic patients needed to prevent one stroke or death with CEA is high at 17 to 32. Can We Improve it ???? 16
Carotid Angioplasty:Fundación Favaloro Experience • Patient Selection: • Traditionally: • Inclusion Criteria: (“anatomic”) • Symptomatic Patients with 70% carotid stenosis. • Asymptomatic Patients 80% carotid stenosis. • Exclusion Criteria. • Patient with dementia or disabling Stroke. • Recent Major Stroke (<30days). Can We Improve Asymptomatic Patient Selection??? Who Benefit More With Revascularization???? 16
Carotid Disease Risk of Stroke in Symptomatic Ptes. • % Stenosis & Risk of Stroke • Plaque Characteristics • 95 % &non Ulcerated 21% • 95 % &Ulcerated 73 % NASCET Ulcerated & Thrombotic Plaque 8
High-Risk Asymptomatic Carotid Stenosis: Ulceration on 3-D Ultrasound vs. Transcranial Doppler Microemboli Prospective analysis of 253 ACS ptes with >60% carotid stenosis Conclusion: The presence of ulcers or microemboli identify Ptes with Asymptomatic carotid stenosis who will benefit from revascularization rather than optimal medical therapy alone. Madani A, et al. Neurology 2011;77:744-750
Silent Cerebral Events in Asymptomatic Carotid Stenosis Aim: to examine the evidence for subclinical microembolization and silent brain infarction in the prediction of stroke in asymptomatic carotid stenosis using transcranial Doppler (TCD), computed tomography (CT), and magnetic resonance imaging (MRI). Outcomes: 58 full text met inclusion criteria. A specific pattern of silent CT infarctions was related to future stroke risk (odds ratio [OR] = 4.6; confidence interval [CI] = 3.0-7.2; P < .0001). There are no prospective MRI studies linking silent infarction and stroke risk. CONCLUSIONS: There is level 1 evidence for the use of TCD to detect microembolization as a risk stratification tool. However, this technique requires further investigation as a stroke prevention tool and would be complemented by improvements in carotid plaque imaging. Jayasooriya G, et al. J Vasc Surg. 2011 Jul;54(1):227-36
Carotid Endartherectomy: Guidelines... Acceptable Morbidity and Mortality.Ad Hoc Committee, AHA. Carotid Interventions: Safety! Symptomatic <6% Asymptomatic <3% ! 17
Global Experience: In-Hospital Outcomes. Procedures 779 Procedural Success (%) 760 (97.5) TIA (%) 12 (1.5) Minor Stroke (%) 15 (1.9) Major Stroke (%)# 12 (1.5) Death (%) (non-related) 5(0.6) Related Death 3 (0.4) Any Stroke & Death (%) 35 (4.5) Carotid Angioplasty – Fundación Favaloro Experience October 1995 – August 2012 Clinical Success: Angiog. success without death, urgent surgery, major stroke or AMI # uno fue cardioembólico
Carotid Angioplasty – Fundación Favaloro Experience October 1995 – July 2012 In-Hospital Results related to previous symptoms: n=779 Symptom Asymptom p Number of Procedures (%) 253(32.5) 526 (67.5) With Distal Protection (%) 216 (85.4) 456 (86.7) 0.7 Procedure Success (%) 241 (95.3) 516 (98.1) 0.02 Major Stroke (%) 9 (3.6) 3 (0.6)0.002 Minor Stroke (%) 6 (2.4) 9(1.7) 0.3 TIA (%) 9 (3.6) 3 (0.6) 0.02 Death (non-related to carotid stenting)21 (0.7) 3 (0.6) 0.5 Related Death 1 (0.4) 2 (0.4) 0.6 Any Stroke or All Death (%) 18 (7.1) 17 (3.2) 0.002 Any Stroke or Related-Death (%) 16 (6.3) 14 (2.7) 0.002
CREST Trial: Stenting vs. Carotid Endarterectomy for Treatment of Carotid Artery Stenosis p=0.03 p=ns p=0.005 p=0.03 Brott TG, et al. N Engl J Med 2010;363:11-23
CAS vs. CEA:Metanalysis and Diversity-Adjusted Trial Sequential Analysis of Randomized Periprocedural death, MI or Stroke CAVEATS: 1-Some of these Trails were done by not well-trained operators for CAS. 2-New Trials, like ACST-2, will repit the same error and bring new wrong conclusions. Banagalore S, et al. Arch Neurol. 2011, Feb;68(2): 172-84
CAS vs. CEA: A Comprehensive Meta-Analysis of Short-Term and Long-Term Outcomes Short term Outcomes for Cranial Nerve Injury Economopoulus KP, et al. Stroke. 2011 Mar;42(3):687-92.
Carotid Disease: classical clinical presentation Carotid Stenosis “Symptomatic”: ~25% “Asymptomatic”: ~75% There are no considerations regarding “functional” status Normal Risk High Risk Normal Risk High Risk ~15% ~10% ~50% ~25% Modified from M Jaff, 2007
Cerebral perfusion have been shown to be impaired in asymptomatic Ptes with severe carotid stenosis 1. Many Asymptomatic Ptes have ischemic defect at CT Scan (~20%) CT scan defect presents in asymptomatic Ptes can predict new events at follow-up when obstruction between 60-99%2. But; what be the impact on neurocognitive functions? No definitive answers……. Asymptomatic??? 1Van der Heyden, t al. EuroIntervention. 2011 Apr;6(9):1091-7. .CT measurement of changes in cerebral perfusion in patients with asymptomatic carotid artery stenosis undergoing carotid stenting prior to cardiac surgery: "proof of principle” 2Kakkos SK, et al, J Vasc Surg. 2009 Apr;49(4):902-9. Epub 2009 Feb 15.Silent embolic infarcts on computed tomography brain scans and risk of ipsilateral hemispheric events in patients with asymptomatic internal carotid artery stenosis.
Postive Test Included: Verbal Memory Tests (RAVLT) RAVLT Delayed Test (RAVLT D) Visual Memory Test (ROCF D) Attention Test (TMT-B) Cognitive Flexibility Test (WCST) Information speed processing Test (IST) Changes in Neuropsychological Performance Following Carotid Artery Stenting in Asymptomatic Patients. • Fundación Favaloro Mendiz O, et al. Journal of Neurosurgery. 2012 Jan;116(1):179-84
Neurocognitive Impact of CAS in Asymptomatic Ptes:CAS 3-Month F-U: Cognitive Tests Outcomes Mendiz O, et al. TCT 2010, oral abstract • Fundación Favaloro Mendiz O, et al. Journal of Neurosurgery. 2012 Jan;116(1):179-84
Revascularization for Asymptomatic Carotid Stenosis • Asymptomatic are not all the same. • All treatment outcomes are improved over the time. • Although carotid revascularization proved to be beneficial in historical series, we can currently identify Ptes who may benefit more using revacularization on top of the best Mx treatment. • So call “Asymptomatic” Ptes may benefit from Carotid Revascularization (CAS) when life expectancy is longer than 5 years
Carotid Artery Stenosis • CAS is safe and effective in Symptomatic and Asymptomatic Ptes. when done by well-trained operators. • CAS can be applied to most of Ptes with favorable anatomy. • CAS has more stroke risk and less MI and cranial nerve injury risk according to current evidence.
Gracias por su atención omendiz@ffavaloro.org