Download
1 / 40
420 likes | 586 Vues
ACST. Asymptomatic Carotid Surgery Trial (ACST) 5-year Results. CTSU, Oxford Clinical Trial Service Unit. ACST. ECST. The European Carotid Surgery Trial (ECST) randomised 3024 “symptomatic” patients to carotid endarterectomy (CEA) or control (CEA to be avoided for as long

E N D
ACST Asymptomatic Carotid Surgery Trial (ACST) 5-year Results CTSU, Oxford Clinical Trial Service Unit
ACST ECST • The European Carotid Surgery Trial • (ECST) randomised 3024 “symptomatic” • patients to carotid endarterectomy (CEA) • or control (CEA to be avoided for as long • as possible) between 1981 and 1994. • ECST results showed that CEA • effectively prevented disabling and fatal • stroke in patients with 70-99% • “symptomatic” stenosis.
ACST ACST: Eligibility • “Tight” carotid artery stenosis in the • index artery • “Asymptomatic”: i.e., no ipsilateral • carotidterritory symptoms of stroke or • transient cerebral ischaemia in past • 6/12 • Doctor & patient both substantially • uncertain about immediate CEA
ACST ACST: Follow-up • Yearly follow-up • Major events (death or stroke) to be • reported to ACST • Duplex ultrasound measurements • requested at each follow-up to 5 years • Data on current drug therapy and blood • pressure
ACST ACST: the world’s largest vascular surgery trial Entry1993 – 2003 3120 patients randomised Immediate CEA Deferral CEA vs (CEA: carotid endarterectomy) (i.e. deferral until CEA seems more clearly needed)
ACST: 3120 patients 126 centres in 30 countries Finland 18 Russia 10 Norway 47 New Zealand: 10 Brazil: 2 Canada: 30 USA: 16 Tunisia: 11 Sweden 532 Netherlands 132 UK 1069 Ireland 7 Czech Republic 18 Poland 88 Belgium 1 Hungary 59 Germany 98 France 2 Yugoslavia 77 Switzerland 6 Bulgaria 6 Austria 30 Italy 328 Israel 245 Cyprus 13 Slovenia 44 Portugal 13 Spain 196 Croatia 2 Greece 10
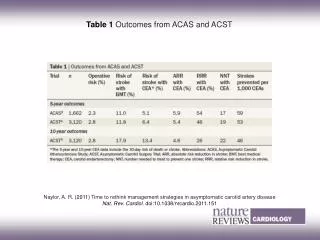
ACST ACST: Baseline data (1) • 1560 allocated immediate CEA • 1560 allocated deferral CEA • Mean follow-up 3.4 years • Baseline characteristics similar to • ACAS (1662 patients, mean follow-up • 2.7 years)
ACST ACST: Baseline data (2) * ACAS: “Has your doctor ever told you you had high blood pressure or were hypertensive?”
ACST Drug therapy at entry (%), by year of randomisation: 1993-1996, 1997-1999 (centre bar), 2000-2003
ACST Medical treatment at 2002/3 follow-up
Proportion with ipsilateral CEA by time from randomisation Ipsilateral CEA (%)
ACST ACST: Numbers undergoing CEA after randomisation
ACST: Surgical mortality and morbidity ACST * Difference between groups in risk per CEA not significant
ACST Perioperative hazards: NO significant differences in CEA risk between male & female; age <65, 65-74, 75+; or any other factor (26 subgroups) But, with data on only 51 perioperative strokes or deaths, such subgroup analyses are unreliable
ACST Carotid territory ischaemic strokes: Laterality and severity (fatal + disabling + not) Excludes periop., & 12 vs 15 haemorrhagic or vertebrobasilar
ACST Which types of patient gain worthwhile benefit from successful CEA? 5-year risks of carotid territory ischaemic stroke
ACST WOMEN: Carotid territory ischaemic strokes within 5 years of randomisation in ACST * Excludes vertebrobasilar or haemorrhagic strokes (2 vs 2)
p<0.0001 Note: cholesterol lowering drug use was low initially but rose substantially
ACST 26 SUBGROUP ANALYSES • No definite heterogeneity of perioperative hazards, • or of proportional reductions by CEA in 5-year risk of • carotid ischaemic stroke • Maybe more benefit for those with cholesterol • >6.5 mmol/l (250 mg/dl), but still significant benefit • for those with lower cholesterol • Maybe less benefit for those aged over 75 (whose • mean age was ~80 and hence had short life • expectancy anyway)
ACST CONCLUSION: NET BENEFIT (AT LEAST UP TO AGE 75) • Overall in ACST, net 5-year risk of stroke • (including perioperative stroke/death): • ~ 6% with Immediate CEA • ~ 12% with Deferred CEA • Difference highly significant (2P = 0.00001) • Benefits significant for men & for women; • for age <65 & for age 65-74; • for ~70% stenosis on ultrasound & for ~80% or ~90% • More needed on which types of patient gain worthwhile • benefit, & on generalisability of findings
ACST CONCLUSION (2): Applicability of findings • The reduction of ~ 4/5 in carotid ischaemic stroke can be generalised to patients with severe carotid artery stenosis in a whole range of future circumstances • Although wider use of statins will somewhat reduce overall risk of carotid stroke, whatever risk remains from the carotid lesion should be avoidable by successful surgery • However, unsuccessful surgery can do much harm. In non-trial settings, unskilled surgeons, inadequate audits or poor selection of patients could result in widespread misuse of CEA
ACST CONCLUSION (3): Applicability of findings • Balance of risk and benefit depends on • - surgical morbidity rates • - risk of carotid stroke in absence of surgery • - what happens after fifth year of follow-up. Continued • divergence between treatment groups suggests • longer observation (to 10 years) could reveal further gain • Until 10-year stroke rates have been monitored, direct estimates of numbers needed to avoid one stroke, expected years of life gained or health economic evaluations are premature, and might undervalue immediate surgery
ACST 2003 – 5-year follow-up2008 – 10-year follow-up
ACST Collaborators’ Meeting 2003 Malmö, Sweden
ACST ACST: Trial Organisation P.I.s: Alison Halliday, Averil Mansfield, Richard Peto, Dafydd Thomas ACST Office: Alison Halliday (PI), Elizabeth Hayter, Dora Kamugasha, Joanna Marro (Trial co-ordinator), Carl Peto (Computing) Steering Committee: John Potter (Chair), Martin Brown, Barbara Farrell, Delyth Morgan (MRC), Angela Rau, Charles Wolfe (+ PIs & ACST office) Audit: Michael Harrison (Chair), Rodney Foale, C Jamieson, Vaughan Ruckley DMC: Charles Warlow (Chair), Rory Collins, Richard Gray, Jean-Marc Orgogozo Clinical Trial Service Unit, Oxford (CTSU): A Baxter, J Burrett R Collins, J Godwin, S Knight, R Peto, A Radley, S Richards