Download

1 / 39
390 likes | 520 Vues
SUNSHINE COAST ACAT. Intake and Community Education. Plan. Do. Act. Check. In 2008 the Sunshine Coast ACAT identified a need to review our intake system. The review was conducted using standard QI processes. Feedback.

E N D
SUNSHINE COAST ACAT Intake and Community Education.
Plan Do Act Check In 2008 the Sunshine Coast ACAT identified a need to review our intake system. The review was conducted using standard QI processes. Feedback A Brainstorming session was held to identify areas for improvement.
THE BRAIN STORMING SESSION IDENTIFIED. • Limited ability to identify sources of inappropriate referral. • No clinical Assessment of most referrals to determine the appropriate timeframe for face to face Assessment. • Even though referees were told to contact ACAT if circumstance change there was a perception this did not occur. • When Contact was made category 3 clients had already been waiting for an extended period – so it seemed inappropriate to cancel referral or refer to another agency at that time if ACAT Assessment not really required.
Project Team • Sponsor – Carol Pass Sunshine Coast ACAT Team Leader. Anne Constant CN Janet Buscombe SW Margaret Monteith SW Karen Austin PT Heather Scott PT Sheryl Scofield OT Kate Websdale CN
OUTCOME OF BRAIN STORMING SESSION • It was decided to trial a new intake system.“ A second intake officer would be rostered on each day to contact all referees to establish purpose and urgency of all referrals.”
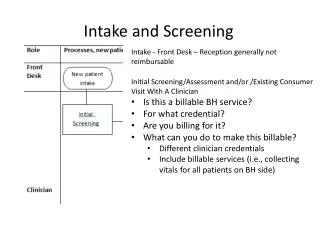
OLD SYSTEM OF INTAKE • Hospital and GP referrals only triaged by one intake officer. • All telephone referrals taken by Admin Staff and referees were told the waiting time for Non Urgent referrals was up to 6 – 8 weeks. They Were asked if this was acceptable, if not these calls were sent to intake for triage.
OLD SYSTEM OF INTAKE Cont: Yes Registered as Cat 3 and allocated. (Referees told to contact ACAT if circumstances changed and the situation became more urgent.) No Referee put thru to intake officer for triage. • All written or faxed referrals designated Cat 3 unless there was anything written to indicate a more urgent timeframe required.
IF NO: • The intake officer would then determine the level of urgency and the referral would be allocated accordingly.
Category 3 referrals once allocated to an assessor often sat in the assessors drawer for up to 8 weeks or more before contact was made and an appointment for assessment arranged.
THIS RESULTED IN • A % of ACAT assessments being completed for inappropriate referrals. • Perpetuation of long waiting times for category 3 referrals. • Risk to clients due to absence of proper triaging. • Assessor stress due to high work loads.
AIM OF NEW INTAKE PROCESS • Better triaging of all referrals to ensure all clients assessed by the most appropriate agency. • Where ACAT is the most appropriate agency time frames for assessment appropriate. • Cancellation or referral on, of inappropriate clients to reduce numbers of people waiting for assessment. • To reduce assessor stress as a result of smaller case loads.
SIDE ISSUE To compliment the new process, the intake system would also identify people who requested ACAT Assessment for future planning purposes only. ACAT would provide group education sessions regularly across our region and future planning clients would be encouraged to attend these sessions rather than have a one on one face to face assessment.
POTENTIAL RISKS OF NEW PROCESS • Client dissatisfaction if they were ‘encouraged’ not to proceed with face to face assessment. • It was calculated that 10 referrals a week had to be cancelled to justify taking 1 FTE assessor off line to do the second intake officer role. If this was not achievable it potentially could increase waiting times for CAT 3 referrals. • There could be a learnt response of indicating a readiness to access care in order to have an assessment. • Benefits of early intervention strategies provided by ACAT lost resulting in increased carer stress and demand for care in the future.
POTENTIAL RISKS OF NEW PROCESS CONT. • Higher incidence of service providers ringing for advice etc prior to putting in referrals. • Inconsistencies of information given/acceptance of referrals between intake officers.
SO • It was decided to trial the new process from May 12th 2008.
EVALUATION WOULD LOOK AT • Impact on waiting times for category 3 referrals. • Number % of referrals found to be inappropriate. • Sources of inappropriate referrals ( to see if education to reduce number of inappropriate referrals was required). • Reasons referrals deemed to be inappropriate.
EARLY EVALUATION 12/5/08 – 15/8/08 Total referrals. 1515 Number of referrals cancelled. 180 Percentage of referrals cancelled 12 %
SOURCE OF REFERRALS CANCELLED NUMBER % • General Practioner 54 30% • Family/ Friend 34 19% • Community Service 28 16% • Self 24 13% • Hospital 19 11% • Specialists 4 2% • Blue Care 11 6% • RACF 3 2% • CRCC 2 1% • DSQ 1 .5%
REASON FOR CANCELLATION Number % • HACC/DVA Services required. 75 42% • Client not consenting. 34 19% • Referral for future planning or ‘Just in case’. 13 7% • Medically unstable / going to rehab. 19 11% • Current approvals in place. 16 9% • Client outside target population. 9 5% • Required another ACAT 4 2% • Referred for Independent Living Unit. 2 1% • CCRC only required. 3 2% • Client died. 1 .5% • Referral was an administrative error. 2 1% • Other – wanted weekly hairdressing, personal alarm. 2 1% • Requires ongoing DSQ support 1 .5%
POSSIBLE STRATEGIES TO REDUCE FUTURE INAPPROPRIATE REFERRALS • Education sessions for service providers. • Community education sessions. • Distribution of resource lists to GP’s through the division of general practice. • District wide access points or central intake service.
NEGATIVE OUTCOMES THAT EMERGED • Increase in category 1 & 2 referrals – this was good for clients but increased service provision difficulties. • The above initially increased waiting time for category 3 referrals. • Significant re referrals of cancelled clients. • Increased dissatisfaction for clients and service providers. • A significant number of people who ‘demanded’ assessment even though there is was no apparent reason to proceed. • A number of clients who travelled through intake to assessment and who were then identified as not having needed assessment.
POSSIBLE POSITIVES THAT EMERGED • 3 Months prior to commencing the new system the average waiting time for Cat 3 was 37days with maximum waiting time 139 days.First 3 months of the new system the average waiting time has dropped to 19 days with a maximum waiting time of 97 days.
WHERE TO FROM THERE • Continue the process. • The value of all clients being triaged was clearly a positive benefit. It was yet to be established as to whether this process would reduce numbers of referrals and waiting times in the long term.
12 MONTH EVALUATION 12/5/08 – 12/5/09 Total Referrals 4496 Number of Referrals Cancelled 670 Percentage of Referrals Cancelled 14.9%
SOURCE OF REFERRALS Cancelled Number % • General Practioner 264 39% • Family/ Friend 116 17% • Community Service 87 13% • Hospital 80 12% • Self 59 9% • Blue Care 34 5% • RACF 22 3% • Specialist 8 1% Source of % remained constant from early evaluation with the exception of Inappropriate referrals from clients and hospitals which switched positions.
STRATERGIES IMPLEMENTED TO ADDRESS THE NUMBER OF INAPPROPRIATE REFERRALS Written feed back to referee with: • Reason the referral was cancelled. • Details of information provided & / or referrals made to other agencies for the client. * Appendix A
REASON FOR CANCELLATION Number % • HACC / DVA Services required 176 26% • Client not consenting 103 15% • Current Approvals in Place 86 13% • Medically Unstable / going to Rehab 66 10% • Domestic help only required 58 9% • Future Planning/just in case referral 54 8% • Client outside target population 44 7% • CCRC only required 18 3% • Wanting ILU or other accommodation not requiring ACAT assessment 13 2?%
REASON FOR CANCELLATION Cont: Number % • Requiring Allied Health Only 12 2% • Out of Geographical Area covered by Sunshine Coast ACAT 8 1% • Referral needed for spouse/partner not referred client 7 1% • Referee withdrew referral 7 1% • Client died 6 1% • Referral an administrative error 6 1% • Unable to contact client 2 <1% • Personal alarm only required 1 <1% • Hair washing only required 1 <1% • Unclear 3 <1%
OTHER PROCESSES NOW IMPLEMENTED TO IMPROVE SERVICE FROM THE INTAKE SYSTEM • All clients Triaged as category 3 receive a letter informing them the referral has been accepted and placed on a waiting list. * Appendix C • The letter requests that they contact ACAT if their circumstances become more urgent. • They also receive the fact sheet about ACAT and a copy of the Australian Charter of HealthCare – Rights. • Any other resource material that might assist is also sent.
OTHER PROCESSES NOW IMPLEMENTED TO IMPROVE SERVICE FROM THE INTAKE SYSTEM CONT: • All clients whose referral is cancelled at intake receive a letter informing them that: • Referral has been cancelled and why. • What recommendations / referrals have been made on their behalf. • The appeals Mechanism as Non Acceptance of a referral is a reviewable decision. * Appendix B
Community Education Sessions • Clients wanting future planning / information are referred to the Community Education Sessions. • Service Providers ( including GP practice staff) are invited to attend Community Education Sessions.
Community Education Sessions Cont: Are held quarterly across the region covered by the Sunshine Coast ACAT. The sessions include: • Information on referral to ACAT • The Intake Process • The Assessment Process • The Continuim of Aged Care Services (HACC, Package Care, Residential Care, Respite Services etc)
SUMMARY AFTER 12/12 EVALUATION • The new intake system provided better client service. Effective triage of all referrals ensures that all clients requiring assessment are assessed in an appropriate timeframe. • All stakeholders receive appropriate feedback if referrals do not proceed to assessment. • Waiting times for not urgent (cat 3) referrals have shortened. • Community education sessions are popular especially with service providers. • Feedback from community eduction evaluations has been very positive.
CONCLUSION The Intake System ensures the client’s referred to ACAT: • Are effectively triaged and seen in appropriate time frames. • Receive timely information on their rights. • Receive relevant information on services that may be useful at the time of intake. • Only appropriate referrals proceed to full assessment. • Clients & service providers receive appropriate feedback.




![Education Workshop [Learning and Community]](https://cdn1.slideserve.com/3428957/education-workshop-learning-and-community-dt.jpg)