Download
1 / 105
1.07k likes | 1.39k Vues
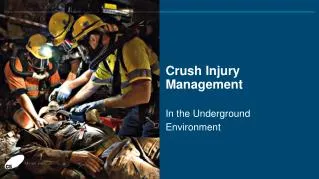
LEARNING FROM DISASTERS (Focus on Nephrology Experience on Crush Syndrome). FILOTEO C. FERRER, MD Section of Nephrology Makati Medical Center March 24, 2011. Outline. Lessons from past disasters (Objectives) Be aware Understand Prepare. SCIENTIFIC METHODOLOGY.

E N D
LEARNING FROM DISASTERS(Focus on Nephrology Experience on Crush Syndrome) FILOTEO C. FERRER, MD Section of Nephrology Makati Medical Center March 24, 2011
Outline • Lessons from past disasters (Objectives) • Be aware • Understand • Prepare
NO EXPERIMENTAL MODEL OF DISASTERS • Only way to collect information and draw conclusions is by: • Retrospective analysis of past disasters • And have a good understanding of these lessons
NO EXPERIMENTAL MODEL OF DISASTERS • Lessons learned from these unfortunate experiences can contribute • Minimize number of mistakes • Implement an effective response • Decrease death toll in future catastrophes
INCIDENCE OF CRUSH INJURY AFTER DISASTRERS • Intensity of the disaster • Population density of the region • Structural characteristics of the buildings • Timing of disaster • Efficacy of rescue
Crush injury is defined as a direct injury caused by collapsing material and debris resulting in manifest muscle swelling and/or neurological disturbances in the affected parts of the body.
Crush Syndrome on the other hand is defined as patients with crush injury and systemic manifestation due to muscle cell damage which would include: • acute kidney injury • Sepsis • acute respiratory distress syndrome • diffuse intravascular coaugulation • Bleeding • hypovolemic shock • cardiac failure • arrhythmias • electrolyte disturbances.
Crush syndrome • Second most frequent cause of disaster related mortality after earthquakes (after direct trauma) • Incidence may increase up to 2-5% overall in disaster victims • But according to general perception: • they constitute a relatively minor group requiring a complex labor- intensive therapeutic measures and are rarely included in governmental or local disaster plans (emergency teams concentrate on housing and primary health ) Sever M.S., et al Renal disaster relief: from theory to practice NDT (2009)
Crush Syndrome (CS) • It takes a lot of effort to extricate victims from the rubble • Hence, it would be deplorable and even counter productive if proper therapeutic possibilities would not be prepared and offered Sever M.S., et al Renal disaster relief; from theory to practice; NDT (2009)
Bywaters described four(4) cases in 1941 1st case seen on Sun. Sept. 16, 1940 at Hammersmith Hosp. 17 yr, old girl with crush injury involving L leg. Initially responded to fluid but became oliguric with rising urea, died suddenly on the 8th day with K 34 mg% (8.7 mEq/L). British Medical Journal 1941 March
Pathophysiology of CS Prolonged pressure on the limbs Ischemic insult (endothelium) Stretch insult (myocytes) Ischemia reperfusion injury -oxygen free radicals -Leukocyte activation -calcium influx -Other body reactions Extreme tension Inc Symp activity Inc cathecholamines RHABDOMYOLYSIS Release of pressure on the limb (rescue) F A S C I O T O M Y Systemic deterioration Hypovolemia Cardiac arrest Hyperkalemia Hypocalcemia ARF DIC,SIRS/MOF Interstitial edema/cell swelling Compartment syndrome myoneuroopathy JMAJ July 2005-Vol 48. 7
Flow of Solutes and water across Skeletal – Muscle- Cell membrane in Rhabdomyolyisis JMAJ July 2005-Vol 48. 7
Flow of Solutes and water across Skeletal – Muscle- Cell membrane in Rhabdomyolyisis
Flow of Solutes and water across Skeletal – Muscle- Cell membrane in Rhabdomyolyisis
TANGSHAN (CHINA) EARTHQUAKEYear: 1976 Intensity 8 Deaths 242K injured 165K CS 2-5 % • Any patient with crush injury is a major casualty • CS patients may suddenly die hyperkalemia
SOUTHERN ITALIAN EARTHQUAKEYear 1980 Intensity 6.8 Deaths 202 CS 19 • Acute Kidney injury was not necessarily observed in all CS victims (12/19= 63%) • Rescued victim who were seemingly well under the rubble deteriorated or even died as soon as after extrication Rescue Death Severe metabolic acidosis Fatal hyperkalemia Santangelo et al Surg and Gyne 1982
Lebanon ExperienceYear 1982 Deaths 80 CS 7 Dialysed 1 Archives of Int Med 1984 : 144 : p277-280
Lebanon ExperienceYear 1982 Deaths 80 CS 7 Dialysed 1 • Immediate fluid resuscitation is of vital importance to prevent crush syndrome complications
ARMENIAN EARTHQUAKEYear: 1988 Intensity 6.8 deaths 25K- 150K CS 600 Dialysis 225 600 cases of AKI, 225 cases of which needed dialysis created second catastrophe/disaster (“RENAL DISASTER”) Despite availability of 36 tons of dialysis supplies, 100 dialysis machines and volunteer personel from many countries the response was ineffective Worsened the chaos “Third disaster “
ARMENIAN EARTHQUAKEYear: 1988 Intensity 6.8 deaths 25K- 150K CS 600 Dialysis 225 • “Disaster within in a disaster” • No organized international structure with appropriate training and deployment strategies Disappointing experience
International Society of Nephrology • Logistic organization to avoid similar problems in the future disasters • Headquarters are informed immediately of all disasters • Logistic support from NGOs such as Medicins Sans Frontieres (MSF) • Since the organization, it had intervened in several disasters (Marmara,Bam,Kashmir,Kobe)
Disaster Chief Disaster Relief Coordinator US Geological Survey detects earthquake Visiting disaster area Assessing extent of the problem Chairperson of RDRTF is informed Asking for Global Support Estimation of the needs for support (i.e., medications, blood products) Decision to intervene Asking for local support Dispatching of scouting team Support offered Accessing of local conditions DISASTER RESPONSE LOCAL COORDINATION GLOBAL COORDINATION Major Steps in Global and Local Coordination of Renal-Disaster Relief Efforts NDT (2009) 24 : 1730 -1735
Renal Disaster Response PREPARATIONS BEFORE DISASTER • Composing Disaster Response Team • Directors • Assessment team members • Rescuers and medical personnel • Organizing Educational activities for • Public • Rescue teams • Non-nephrological medical personnel • Nephrological (para) medical personnel • Chronic dialysis patients • Planning the interventions • External planning and preparations • Local planning • Overall disaster planning • Material planning • Planning of dialysis services • Collaboration with external bodies MEASURES AFTER DISASTER • External Intervention • Local Intervention • The acute phase (action plan) • The maintenance phase Major Steps in Renal Disaster Response NDT (2009) 24 : 1730 -1735
PSN DISASTER RESPONSE TO CRUSH INJURY/CRUSH SYNDROME • The Philippines being situated in the Pacific ring of fire is at increased risk of major earthquakes. • Situated in a geotectonically active region
PSN DISASTER RESPONSE TO CRUSH INJURY/CRUSH SYNDROME The1,200-km-long Philippine fault zone (PFZ) is a major tectonic feature that transects the whole Philippine archipelago from northwestern Luzon to southeastern Mindanao. This arc-parallel, left-lateral strike slip fault is divided into several segments and has been the source of large-magnitude earthquakes in recent years, such as the 1973 Ragay Gulf earthquake (M 7.0), 1990 Luzon earthquake (Mw 7.7) , and 2003 Masbate earthquake (Ms 6.2).
Northern Luzon EarthquakeYear 1990 Intensity 7.7 Deaths > 1000 CS ?? AKI ?? • Doctors working under umbrellas and sheets of plastic had treated nearly 800 of the injured • ? Medical publications/experience • Philvolcs and DOST has been mapping the 1200 Km fault zone • Greatly improved earthquake monitoring system from 12 stations now we have 66 seismic stations nationwide,release announcement in less than 10 minutes
PSN DISASTER RESPONSE TO CRUSH INJURY/CRUSH SYNDROME • Most doctors and even nephrologists have no regular experience with CS • Thus, there is a need for guidance • “recommendations only” due to lack of evidence
PRE-EXTRICATION MANAGEMENT OF POTENTIAL CRUSH INJURY VICTIM Immediate fluid resuscitation is of vital importance to prevent crush syndrome complications PSN Disaster Response to CRUSH Injury
POST-EXTRICATION MANAGEMENT OF POTENTIAL CRUSH INJURY VICTIM (PRE-HOSPITAL PHASE) • Any patient with crush injury is a major casualty • CS patients may suddenly die Avoid K containing fluid !!! PSN Disaster Response to CRUSH Injury
VICTIM MAY BE DISCHARGED WITH PROPER ADVICE Victims who are deemed stable with no signs of dehydration, and without significant risk for crush injury/crush syndrome may be discharged or sent home due to limitation of hospital beds should be instructed to: • watch for their color of urine (dark-colored or reddish-colored urine) • monitor the volume of urine (Note for oliguria <400 ml/24 hours) • Watch-out-for symptoms of crush syndrome such as acute weight gain, edema, dyspnea, Seek medical care as soon as possible
POST-EXTRICATION MANAGEMENT OF POTENTIAL CRUSH INJURY VICTIM Once the victim is admitted to the hospital, a thorough ‘comprehensive secondary survey’ is done which includes complete history taking, detailed physical examination and reassessment of all vital signs. (HOSPITAL PHASE) PSN Disaster Response to CRUSH Injury
POST EXTRICATION MANAGEMENT (HOSPITAL PHASE): Continue Hydation: May shift NSS to Alkaline saline hydration: 1L half-isotonic saline with 50 meqs NaHCO3 every 2nd or 3rd cycle of 1L isotonic saline at 0.5 – 1L/hr -theoretically ideal fluid to use as alkalinization of plasma may reduce plasma K and eventually the urine to promote uric acid excretion and increase solubility of myoglobin - but may also promote calcium phosphate deposition inducing or worsening manifestation of hypocalcemia Closely monitor patients and adjust IVF rate accordingly
POST EXTRICATION MANAGEMENT (HOSPITAL PHASE): Continue Hydation: OR May just continue NSS 0.5- 1 lit/day ( If laboratory monitoring is not possible and HCO3 solution is not available) Closely monitor patients and adjust IVF rate accordingly
Bingol (Turkey) EarthquakeYear 2003 Intensity 6.4 Deaths 177 CS 16 Dialysis 4
Bingol (Turkey) EarthquakeYear 2003 Intensity 6.4 Deaths 177 CS 16 Dialysis 4 • Early adequate fluid administration helps prevent dialysis
Bam Iran EarthquakeYear2003 Intensity 6.6 Deaths 25K Injured 30K AKI defined as crea > 1.6 mg/dl or dialysis need
Kobe (Hanshin-Awaji) Japan EarthquakeYear 1995 Intensity 7.2 Deaths 5325 CS 372 AKI 202 Dialysed 123 • Mortality in patients with AKI • Overall 24 .8 % (50 deaths out of 202) • Mortality in patients with AKI and dialysed • 41% ( 50 out of 123 needed dialysis) Most of these patients received only 2 to 3 liters per day during the initial 3 days The journal of trauma 42 (3) March 1997
Marmara EarthquakeYear 1999 Intensity 7.4 Deaths 17K Injured 44K AKI 639 Dialysed 477 • Mean volume of fluid given on the first day of admission : 5109+/- 1711 ml • Survivors vs. non survivors: NS • Dialyzed: 5407+/- 1623 ml • VS. • Non dialyzed : 3825+/- 1539 ml P=.01
Marmara EarthquakeYear 199 Intensity 7.4 Deaths 17K Injured 44K AKI 639 Dialysis 477 • Many victims were admitted to reference hospitals may have already established ATN • Conservative fluid management for late rescued victims to avoid fluid overload and need for dialysis
POST EXTRICATION MANAGEMENT (HOSPITAL PHASE): Conservative Hydration: if close monitoring is impossible late rescued victims as ATN have developed already
The following factors should be considered in hydration • age • (Caution should be exercised in the elderly.) • body mass index • (More fluid is needed for the victims with larger body mass.) • trauma pattern • (More fluid is needed in patient with third spacing) • Edema due to compartment syndrome does not necessarily reflect fluid overload.) • amount of presumed fluid loss • (More fluid should be given to victims with bleeding, and in those in hot climates) • position of the victim • (Those who are on upside down or in a prone position are at higher risk of developing respiratory difficulties following aggressive fluid resuscitation.)
Renal Disaster Response PREPARATIONS BEFORE DISASTER • Composing Disaster Response Team • Directors • Assessment team members • Rescuers and medical personnel • Organizing Educational activities for • Public • Rescue teams • Non-nephrological medical personnel • Nephrological (para) medical personnel • Chronic dialysis patients • Planning the interventions • External planning and preparations • Local planning • Overall disaster planning • Material planning • Planning of dialysis services • Collaboration with external bodies MEASURES AFTER DISASTER • External Intervention • Local Intervention • The acute phase (action plan) • The maintenance phase Major Steps in Renal Disaster Response NDT (2009) 24 : 1730 -1735
Marmara EarthquakeYear 199 Intensity 7.4 Deaths 17K Injured 44K AKI 639 C Dialysis 477 Sever MS, et al, NEJM 2006;354:1052-63