UTERINE RUPTURE
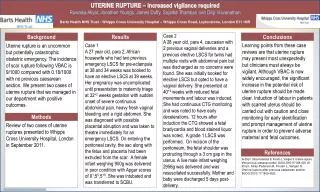
Disruption of the uterine wall any time beyond the 28 th weeks of pregnancy is called Rupture Uterus. Dissolution in the continuity of the Uterine wall any time beyond 28 th weeks of pregnancy is called rupture of the Uterus. It is an Obstetrical emergency.


UTERINE RUPTURE
E N D
Presentation Transcript
Disruption of the uterine wall any time beyond the 28th weeks of pregnancy is called Rupture Uterus. • Dissolution in the continuity of the Uterine wall any time beyond 28th weeks of pregnancy is called rupture of the Uterus. • It is an Obstetrical emergency. • Incidence :- Widely varies from 1 in 2000 to 1-200 deliveries. • Types :- • 1) Complete rupture : All the three layers of the uterus are involved. • 2) Incomplete Rupture: Peritoneum remain intact. UTERINE RUPTURE .
UTERINE RUPTURE • A spontaneous or traumatic rupture of the uterus ie., the actual separation of the uterine myometrium/ previous uterine scar, with rupture of membranes and extrusion of the fetus or fetal parts into the peritoneal cavity. • Dehiscence is the partial separation of the old uterine scar; the fetus usually stays inside the uterus and the bleeding is minimal when dehiscence occurs.
RISK FACTORS: • Women who have had previous surgery on the uterus (upper muscular portion) • Having more than five full-term pregnancies • Having an overdistended uterus (as with twins or other multiples) • Abnormal positions of the baby such as transverse lie. • Use of Pitocin (oxytocin) and other labor-induced medications (prostaglandin) • Rupture of the scar from a previous CS delivery/hysterectomy. • Uterine/abdominal trauma • Uterine congenital anomaly • Obstructed labor; maneuvers within the uterus • Interdelivery interval (time between deliveries)
PATHOPHYSIOLOGY • Women who have had previous surgery on the uterus (upper muscular portion) • Having more than five full-term pregnancies • Having an overdistended uterus (as with twins or other multiples) • Abnormal positions of the baby such as transverse lie. • Use of Pitocin (oxytocin) and other labor-induced medications (prostaglandin) • Rupture of the scar from a previous CS delivery/hysterectomy. • Uterine/abdominal trauma • Uterine congenital anomaly • Obstructed labor; maneuvers within the uterus • Interdelivery interval (time between deliveries) Pathologic retraction ring occurs, strong uterine contractions w/o cervical dilatation “tearing sensation” Complete rupture Incomplete rupture Rupturing of endometrium, myometrium and perimetrium Rupturing of endometrium and myometrium
Uterine contraction stops Localized tenderness and persisting aching pain over the area of the uterine segment • Swelling of the abdomen: • Retracted uterus • Extrauterine fetus Bleeding into the peritoneal cavity Hemorrhage from torn uterine arteries Bleeding to the vagina Decreased blood volume Decreased cardiac output Heart attempts to circulate remaining blood volume Decreased venous return Decreased BP Vasoconstriction of peripheral vessels, increased heart rate
Increases gas exchange to oxygenate better the decreased blood volume Cold, clammy skin Increased respiratory rate Continued blood loss will continue to fall BP Uterine perfusion is decreased Fetal distress Decreased brain perfusion Decreased kidney perfusion Decreased LOC (lethargy, coma) Decreased urine output Renal failure Death of Mother and fetus
ASSESSMENT • Evaluate maternal vital signs; especially note an increase in rate and depth of respirations, an increase in pulse , or a drop in BP indicating status change. • Observe for signs and symptoms of impending rupture (ie, lack of cervical dilatation, tetanic uterine contractions, restlessness, anxiety, severe abdominal pain, fetal bradycardia, or late or variable decelerations of the FHR). • Assess fetal status by continuous monitoring. • Speak with family, and evaluate their understanding of the situation.
SIGNS AND SYMPTOMS: Clinical Manifestations Clinical manifestations depend on the type of rupture, with the possibility that the clinical picture may develop over several hours. Developing Rupture Abdominal pain and tenderness Uterine contractions will usually continue but will diminish in intensity and tone. Bleeding into the abdominal cavity and sometimes into the vagina. Vomiting Syncope; tachycardia; pallor Significant change in FHR characteristics – usually bradycardia (most significant sign)
Violent Traumatic Rupture Sudden sharp abdominal pain during or between contractions. Abdominal tenderness Uterine contractions may be absent, or may continue but be diminished in intensity and cord bleeding vaginally, abdominally, or both Fetus easily palpated in the abdominal with shoulder pain Tenses, acute abdominal with shoulder pain Signs of shock Chest pain from diaphragmatic irritation due to bleeding into the abdomen.
NURSING DIAGNOSIS AND INTERVENTIONS: • Deficient Fluid Volume related to active fluid loss from hemorrhage • Start or maintain an IV fluid as prescribed. Use a large gauge catheter when starting the IV for blood and large quantities of fluid replacemnt. • Maintain CVP and arterial lines, as indicated for hemodynamic monitoring. • Maintain bed rest to decrease metabolic demands. • Insert Foley catheter, and moniter urine output hourly or as indicated. • Obtain and administer blood products as indicated.
Fear related to surgical outcome for fetus and mother • Give brief explanation to the woman and her support person before beginning a procedure. • Answer questions that the family or woman may have. • Maintain a quiet and calm atmosphere to enhance relaxation. • Remain with the woman until anesthesia has been administered; offer support as needed. • Keep the family members aware of the situation while the woman is in surgery and allow time for them to express feelings.
Ineffective Tissue Perfusion, Maternal Vital Organ and Fetal r/t Hypovolemia • Administer O2 using a face mask at 8-12 L/min or as ordered to provide high oxygen concentration. • Apply pulse oximeter, and monitor oxygen saturation as indicated. • Monitor ABG levels and serum electrolytes as indicated to assess respiratory status, observing for hyperventilation and electrolyte imbalance. • Continually monitor maternal and fetal vital signs to assess pattern because progressive changes may indicate profound shock.
Fear r/t Surgical Outcome for Fetus and Mother • Give a brief explanation to the woman and her support person before beginning the procedure. • Answer questions that the family and woman may have. • Maintain a quiet and calm atmosphere to enhance relaxation. • Remain with the woman until anesthesia has been administered; offer support as needed. • Keep the family members aware of the situation while the woman is in surgery and allow time for them to express feelings.
Risk for Infection related to surgical incision • Observe for localized signs of infection. • Cleanse incision or insertion sites daily and PRN with povidone iodine or other appropriate solutions. • Change dressings as needed or indicated. • Encourage early ambulation, deep breathing, coughing and position changes. • Maintain adequate hydration and provide. • Provide perineal care.
MEDICAL MANAGEMENT: • Immediate stabilization of maternal hemodynamics and immediate caesarean delivery • Oxytocin is given to contract the uterus and the replacement . • After surgery, additional blood, and fluid replacement is continued along with antibiotic theory.
SURGICAL MANAGEMENT: • Caesarean Section • Laparotomy • Hysterectomy
NURSING MANAGEMENT: • Continually evaluate maternal vital signs; especially note an increase in rate and depth of respirations, an increase in pulse , or a drop in BP indicating status change. • Assess fetal status by continuous monitoring. • Speak with family, and evaluate their understanding of the situation. • Anticipate the need for an immediate caesarean birth to prevent rupture when symptoms are present. • Provide information to the support person and inform him or her about fetal outcome, the extent of the surgery and the woman’s safety. • Let the pt express her emotion without feeing threatened.