Sinus Pathology
Sinus Pathology. Paranasal sinuses. Staging criteria: primary tumor (T) {AJCC} from Cummings.please see handouts as well for updated AJCC Tx Minimum requirements to assess primary tumor cannot be met T0 No evidence of primary tumor TIS Carcinoma in situ

Sinus Pathology
E N D
Presentation Transcript
Paranasal sinuses • Staging criteria: primary tumor (T) {AJCC} from Cummings.please see handouts as well for updated AJCC • Tx Minimum requirements to assess primary tumor cannot be met • T0 No evidence of primary tumor • TIS Carcinoma in situ • T1 Tumor confined to antral mucosa of infrastructure with no bone erosion or destruction • T2 Tumor confined to suprastructure mucosa without bone destruction, or to infrastructure with destruction of medial or inferior bony walls only • T3 More extensive tumor invading skin of cheek, orbit, anterior ethmoid sinus, or pterygoid muscle • T4 Massive tumor with invasion of cribriform plate, posterior ethmoid sinus, sphenoid sinus, nasopharynx, pterygoid plate, or base of skull
Inflammatory polyp. • Inflammatory polyp. • The medium-power microscopic appearance of this lesion is characteristic of a nasal inflammatory polyp. Note the edematous connective tissue filled with numerous eosinophils (bright pink granules) and plasma cells (blue cells with eccentric round nuclei and perinuclear pink zone in the cytoplasm). The overlying respiratory-type epithelium shows some reactive expansion (hyperplasia) of the basal cell layer but the overlying ciliated epithelial cells are still present.
Inverted papillomas • Inverted papillomas and exophytic squamous papillomas are both characterized by proliferations of the same type of epithelium. In inverted papillomas, this epithelium characteristically grows down into edematous stroma . As the abnormal epithelium continues to expand below the surface, it causes a broad-based mucosal elevation.
RHINOSPORIDIOSIS • Rhinosporidium seeberi . • Rhinosporidiosis occurs in the Americas, Europe, Africa, and Asia but is most common in the tropics, with the highest prevalence in southern India and Sri Lanka. • R. seeberi is visualized with fungal stains such as methenamine silver and Periodic acid-Schiff, as well as mucicarmine
chordoma • "Large cells with multiple vacuoles are called 'physaliferous cells' because of a resemblance to jellyfish. • These neoplasms arise from remnants of primitive notochord .
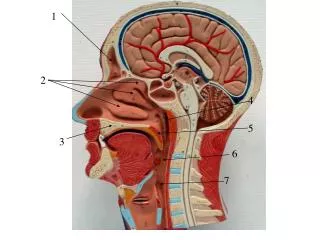
clival chordoma • clival chordoma, depicting tumor and cranial nerve relationships prior to resection of the petrous apex and removal of the tumor.
Squamous papilloma • Squamous papilloma • These are finger-like structures that project into the air passages above the surrounding mucosa. They are surfaced by abnormally thick, non-keratinizing stratified squamous epithelium. The epithelial cells are arranged in an orderly pattern and they do not have the cytologic features of malignancy.
Carcinoma arising in a papilloma • Carcinomas may arise within a preexisting papilloma or directly from non-papillomatous epithelium. All of the epithelial cells here have malignant cytologic features (nuclear enlargement, variability in size and shape) and they are arranged in a disorganized growth pattern. • A most important feature is that these abnormal cells have invaded the connective tissue where they infiltrate as small irregular nests and even as individual cells. Contrast this growth pattern with the smooth, expansile epithelial proliferations in the inverted papilloma. • Infiltration area
Invasive squamous cell carcinoma • Contrast the normal surface squamous epithelium with that of the adjacent invasive carcinoma. This tumor is classified as a squamous cell carcinoma because some of the tumor cells exhibit recognizable squamous differentiation (note the glassy pink nests of keratinized malignant cells within the tumor). Keratinizing and non-keratinizing squamous cell carcinomas may arise anywhere from the nasal vestibule to the lung as well as inside the oral cavity.
Nasopharyngeal carcinoma. • 3 types. • WHO. • I keratinizing, • II nonkeratinizing, • III undifferentiated subtypes (this slide)
Ameloblastoma • The ameloblasts are the palisaded cells with the nuclei pulled away from the basement membrane REVERSED POLARIZATION around a stellate reticulum like tissue and in a fibrous stroma . • REVERSED POLARIZATION.
Ameloblastoma • Cystic lesions