Download
1 / 24
240 likes | 412 Vues
Policy and programme lessons from the Multi-Country Evaluation (MCE) of IMCI. The MCE Team. Malnutrition 52%. MCE Objectives. Document IMCI implementation Measure IMCI impact on health and nutrition Evaluate the cost-effectiveness of IMCI Provide feedback to policy makers.

E N D
Policy and programme lessons from the Multi-Country Evaluation (MCE) of IMCI The MCE Team
Malnutrition 52%
MCE Objectives • Document IMCI implementation • Measure IMCI impact on health and nutrition • Evaluate the cost-effectiveness of IMCI • Provide feedback to policy makers
Major impact on child health and nutrition was expected at country level Introduction of IMCI Family and community interventions Training of health workers Health system improvements Improved quality of care in health facilities Improved careseeking & utilization Improved preventive practices Improved household compliance/care Increased coverage for curative & preventive interventions Improved health/nutrition Reduced mortality
MCE in-depth studies • Bangladesh: • efficacy RCT of 10 IMCI x 10 comparison areas • Tanzania: • pre-post comparison of 2 IMCI x 2 comparison districts • Brazil: • comparison of 32 IMCI x 32 comparison municipalities • Uganda: • pre-post dose-response analysis of IMCI strength of implementation in 10 districts • Peru: • as in Uganda, for 25 departments
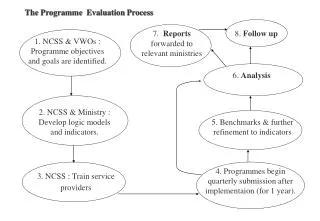
MCE step-wise approach • Are adequate services being provided? • at health facility level? • at community level? • Are these services being used by the population? • Have adequate coverage levels been reached in the population? • Is there an impact on health and nutrition?
IMCI leads to improvementsin health worker performance Source: Paryio G, Schellenberg J et al
And can improve care quality at no extra cost Results from the Brazil MCE confirm that IMCI does not cost more than routine care
Is IMCI being provided at health facility level? • High training coverage has been reached in defined geographical areas • Quality of training is usually good • Difficulties in going to scale in relation to staff turnover and maintaining of quality of training • Need for health systems support • Drugs • Supervision • Referral • District management skills
Utilization is often too low to achieve impact through facility-based services alone % sick children who were taken first to a government facility Source: Arifeen S, Paryio G, Schellenberg J et al
In Bangladesh, IMCI is associated with increases in health facility utilization Data source: MCE-Bangladesh, Routine MIS and GoB MIS But no other MCE site was able to replicate this effect……
But coverage for key community interventions remains low in most countries Population coverage for key family practices Uganda MCE – 10 districts Source: Paryio G et al
In Peru, facility and communityIMCI were not implementedin the same departments Departmental coverage of IMCI-trained clinical and community workers (2003) Similar results in Tanzania Each dot representsone department Source: Huicho L et al
Is IMCI being provided at community level? • Implementation is spotty and uncoordinated with health worker training • Community case-management interventions not included • Community IMCI includes too many messages • These findings have helped generate increased focus on the implementation of community component of IMCI
Tanzania: underfive mortalitywas 13% lower in the two IMCI districts Significant impact on stunting Full IMCI in HF 13% difference 95% CI: -7%, 30% End of study Source: Schellenberg J et al
IMCI: No apparent impact in Peru r= 0.048 P= 0.824 Similar results in Brazil and Uganda
Summing up (1) • IMCI improves quality of care • IMCI does not increase overall costs • Either for providers or out-of-pocket • IMCI dramatically reduces cost per child managed correctly • IMCI is the gold standard for facility care of children aged 7 days – 5 years
Summing up (2) • IMCI can have an impact on mortality and nutrition • But this requires: • Strengthening health systems • Reaching out to the community • IMCI was least likely to be implemented well where it was needed most
What the MCE has contributed • Feedback at national level • Repositioning IMCI in the context of child survival by WHO and other agencies • Lancet Child Survival Series + 30 papers • Increased advocacy for child survival
What the MCE has contributed • The MCE showed that having interventions is not enough • The real challenge is how to deliver these interventions to those who need them most
From MCE we know IMCI works in facilities! Requires adequate attention to health systems support and community coverage MCE was not able to evaluate the effectiveness of the community component of IMCI IMCI, as originally constructed, may not be the answer in every setting IMCI is evolving! IMCI and child health
Since these results first came out, IMCI has been scaled up to almost a fifth of Bangladesh, especially in high mortality areas Quality of training and performance outcomes have been maintained Initial focus on facility-based services, with increasing inclusion of health systems support and community interventions Shift from strategy to programme Scaling up IMCI The Bangladesh experience
IMCI and child health CHILD HEALTH AND NUTRITION STRATEGY IMCI