Chronic Kidney Disease Prevention Strategies
610 likes | 818 Vues
Learn about risk factors, prevention methods, and lifestyle modifications to combat chronic kidney disease (CKD) and its complications. Community health education, screening programs, and awareness initiatives play a crucial role in preventing CKD. Engage with healthcare professionals and community members for effective prevention strategies.

Chronic Kidney Disease Prevention Strategies
E N D
Presentation Transcript
RRT 2,095,000 1,065,000 426,000 1990 2010 2000 Lysaght, J Am Soc Nephrol, 2002
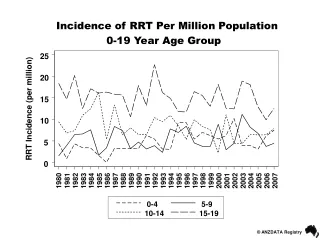
Adjusted incident rates & annual percent changeFigure 2.2 Incident ESRD patients; Medical Evidence form data; rates adjusted for age, gender, & race.
There are 1,065,000 people on dialysis worldwide 90 % of them live in North America, Japan, and Europe, whose population is less than 20 % of world population
K/DOQI CKD Classification Stage Description GFR 1 Kidney damage/normal GFR >90ml/min 2 Mild renal insufficiency 89-60 3 Moderate renal insufficiency 59-30 4 Severe renal insufficiency 29-15 5 Kidney Failure <15
PRE-CKD X CKD 1 X CKD 2 CKD3 CKD4 X ESRF
PRE-CKD CKD 1 CKD 2 CKD3 AT RISK CKD4 ESRF
Risk Factors in CKD S P I Genetic/Relatives of CKD Race Gender Age Diseases: DM, HT, auto-immune, Rheumatic Infections: Malaria, HIV, HCV, Streptococcus
USA UK
Risk Factors in CKD S I P BP Glycaemia Dyslipidemia Weight Smoking INFECTIONS: HCV, HIV, Malaria, schisto
PRE-CKD Established CKF CKD 1 CKD 2 CKD3 CKD4 ESRF
Risk Factors in CKD S I P Modifiable BP Proteinuria Dyslipidemia Smoking
DN Non-DN Orth 2002
PRE-CKD Established CKF CKD 1 CKD 2 CKD3 CKD4 ESRF
Proteinuria <1g/d Hypertension <125/75 Alcohol Lipids <5 Weight Smoking STOP
ACEI/ARB NDCCB Renoprotection ACEI/ARB NDCCB b-blocker STATIN STOP Cardioprotection
PRE-CKD X CKD 1 X CKD 2 CKD3 CKD4 X ESRF
ESRD Lack of resources Lack Nephologists Lack Dialysis GUIDELINES Death
What to do???????? • Community Health Education and Awareness Programmes (CHEAP) • Screening programmes • Train a new generation of Nephro-epidemiologists • Inform General practitioners • Train Community Health Work Assistants • Engage communities, NGO and Pharmaceutical industry
PRE-CKD CKD 1 CKD 2 CKD3 AT RISK CKD4 ESRF
K/DOQIAt-risk Population + CKD 1 • At-risk Population • DM, HT • Obese individuals • Relatives of CKD • Ethnic/racial populations at risk • Infections: malaria, Schisto, HCV, HIV
DM Prevent PREVENTION Screen Treat
IGT 2000:197m 2025:380m DM 2000:155m 2025: 300m DN 2000:15-30m 2025:30-60m
Obesity/Glucose intolerance Da Qing IGT and Diabetes Study (Pan et al, 1997) Exercise (4h/week) Diet Diet + exercise Diabetes Prevention Programe (Molitch et al 2003) Metformin v Lifestyle modification Finnish Diabetes Prevention Study (Lindstrom et al, 2003) Lifestyle
Obesity/Glucose intolerance Da Qing IGT and Diabetes Study (Pan et al, 1997) Exercise (4h/week) -36% Diet -31% Diet + exercise -42% Diabetes Prevention Programe (Molitch et al 2003) Metformin -31% Lifestyle modification -58% Finnish Diabetes Prevention Study (Lindstrom et al, 2003) Lifestyle -58%
Diabetes prevention « if everybody exercised few hours a week, type 2 diabetes would be virtually nonexistent » Ken Goodrick M.D. (Baylor College of Medicine)TIME 5 February 2001
HT Prevent PREVENTION Screen Treat
Lifestyle Modifications & CKD • Salt Restriction • Weight Reduction • Exercise
DASH-Salt Na: 141 mmol/d Na: 106 Na: 65
PRE-CKD CKD 1 CKD 2 CKD3 CKD4 ESRF
What to do???????? • Community Health Education and Awareness Programmes (CHEAP) • Screening programmes • Inform General practitioners • Train a new generation of Nephro-epidemiologists • Train Community Health Work Assistants • Engage communities, NGO and Pharmaceutical industry
K/DOQIAt-risk Population + CKD 1 • At-risk Population • DM, HT • Obese individuals • Relatives of CKD • Ethnic/racial populations at risk • Infections: malaria, Schisto, HCV, HIV