Download
1 / 77
1.07k likes | 2.62k Vues
Ventilatory Care of Critically ill Patient and Weaning from Mechanical Ventilation. Dr Priyanka. University College of Medical Sciences & GTB Hospital, Delhi. Contents. Introduction Stages of weaning Weaning criteria Weaning procedure Weaning protocols

E N D
Ventilatory Care of Critically ill Patient and Weaning from Mechanical Ventilation Dr Priyanka University College of Medical Sciences & GTB Hospital, Delhi
Contents • Introduction • Stages of weaning • Weaning criteria • Weaning procedure • Weaning protocols • Pathophysiology of weaning failure • Specialised weaning units (SWUs)
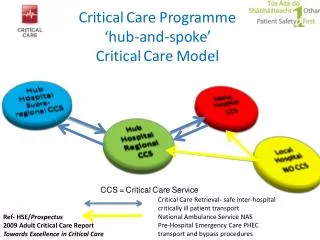
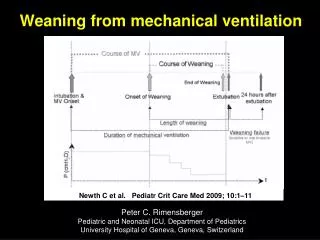
Weaning • Process of withdrawal of mechanical ventilatory support that transfers the work of breathing from ventilator to the patient • This period may take many forms ranging from abrupt to gradual withdrawal from ventilatory support • The aim of ventilatory support is to unload the patient’s respiratory pump, while weaning is the process of reloading the respiratory pump
75% of mechanically ventilated patients are easy to be weaned off the ventilator with simple process • 10-15% patients require use of a weaning protocol over a period of 24-72 hours • 5-10% require a gradual weaning over longer time • 1% of patients become chronically dependent on ventilator • Out of the total time that a patient spends on ventilator, 40% of the time is spent on weaning process
Decreases the availability of ICU beds Increased cost Increased hospital length of stay Increased risk of VAP Why Wean early ??? Increased ICU length of stay Increased morbidity & mortality Can adversely affect the patient outcome
Different stages Of Weaning in Mechanically Ventilated pts failure should be avoided whenever possible because the need for reintubation carries an 8-fold higher odds ratio for nosocomial pneumonia99 and a 6-fold to 12-fold increased mortality risk. reintubation rates range from 4 to 23% for different ICU populations In contrast, the maintenance of unnecessary ventilator support carries its own burden of patient risk for infection and other complications 1. Treatment of ARF 3. Assessing readiness to wean 5. Extubation 6. Reintubation 2. Suspicion 4. SBT Admit Discharge
Evaluating Patients to Be Weaned from Mechanical Ventilator A daily routine follow up should be done in every patient receiving mechanical ventilation and exploring the following condition • Resolution/improvement of the underlying disease • Stop sedation • Core temperature below 38 ºC • Stable haemodynamics (HR < 140/min, stable BP) with no/minimal need of vasoactive drugs, absence of active myocardial ischemia • Adequate haemoglobin (Hb > 8 g/dL) • Adequate mentation (arousable, GCS > 13) • No major metabolic and/or electrolyte disturbances
Weaning Criteria Clinical Criteria Objective Criteria Adequate cough Absence of excessive tracheobronchial secretions Resolution of the disease acute phase for which the patient was intubated Ventilatory criteria Oxygenation criteria Pulmonary reserve Pulmonary measurements Other factors
Ventilatory Criteria • PaCO2 < 50 mmHg with normal pH • Vital Capacity > 10 to 15 ml/kg • Spontaneous VT > 5 to 8 ml/kg • Spontaneous RR < 30/min • Minute ventilation < 10 l/min PaCO2 – most reliable indicator VC and spon VT – indicate mechanical cond of lungs A high spon RR and MV indicate ↑ WOB
Oxygenation Criteria • PaO2 > 60 mmHg @FiO2 < 0.4, PEEP < 5 cm H2O • SaO2 > 90% @ FiO2< 0.4 • PaO2/FiO2 > 200 mmHg • P(A-a)O2 < 350 mmHg (corresponds to 14% shunt) • Qs/Qt < 20% Qs/Qt estimate wasted pulmonary perfusion P(A-a)O2 is related to degree of hypoxemia/shunt In pts with anemia or dysfunctHb, PaO2 and SaO2 don’t reflect true oxygenation status So arterial oxygen content should be measured
Pulmonary Reserve Pulmonary reserve requires active pt cooperation Pulmonary measurements indicate workload needed to support spont. ventilation • Max. voluntary ventilation 2× MV@FiO2 upto 0.4 • Max. Insp. Pressure (MIP) < -20 to -30 cmH2O
Pulmonary measurements • Static compliance > 30 ml/cm H2O • Airway resistance observe trend • Vd/Vt < 0.6
Weaning is more likely to succeed if a patient meets most of the criteria. If a patient can meet only one or two of the weaning criteria, the success rate is likely to be low. Though not fool proof, all patients who fit most of the criteria can undergo a formal spontaneous breathing trial (SBT).
Combined weaning indices Since respiratory failure is multifactorial individual predictors may be unrelaible predictors of weaning outcome Since respiratory failure is multifactorial, individual parameters are unreliable predictors of weaning outcome Indices integrating several physiological variables may be more effective predictors of weaning outcome • RSBI (Rapid shallow breathing index) • CROP Index • SWI Index
RSBI ( Rapid shallow breathing index) • Index of rapid and shallow breathing f/Vt • RSBI<105 predicts successful weaning attempts • First described by Yang and Tobin in 1991 • The RSBI measurement is performed immediately after discontinuation of ventilatory support with the patient still intubated and spontaneously breathing room air for 1 min • More accurate predictor of weaning success than any other parameter studied • Disadvantage: excessive false +ve
RSBI Rate • A measure of change of RSBI over time • Calculated by obtaining the difference between the initial RSBI and the final RSBI, and then dividing the result by the initial RSBI. The resulting number is then multiplied by 100. • RSBI Rate = [(RSBI2 – RSBI1)/RSBI1] x100 • It was shown that RSBI Rate of less than 20% was over 90% sensitive and 100% specific for predicting weaning success.
CROP Index( Compliance Rate Oxygenation Pressure Index) Evaluates pulmonary gas exchange and balance b/w respiratory demands and respiratory neuromuscular reserve CROP Index= ( Cd × MIP × PaO2/PAO2)/f • Where Cd = dynamic compliance MIP= maximum inspiratory pressure PaO2 = Arterial oxygen tension PAO2 = Alveolar oxygen tension f = spontaneous respiratory rate per minute • Should be > 13 ml/breath/min for successful weaning • Widespread application limited by complicated calculation & no. of variables involved
SWI (Simplified Weaning Index) Evaluates efficiency of gas exchange and ventilatory endurance SWI = ( fmv (PIP – PEEP)/MIP) × PaCO2/40 • Where PIP = peak inspiratory pressure PEEP = Peak end expiratory pressure MIP = Maximal inspiratory pressure fmv = ventilatory frequency PaCO2 = Arterial CO2 tension while on ventilator • Value < 9/min → successful weaning outcome
Other Criteria P 0.1 (Maximal occlusion pressure) • Airway occlusion pressure measured 100 msec after a maximal inspiratory effort against an occluded airway • It is effort independent and correlates well with central respiratory drive • Patients with P0.1 >6 cm H2O tend to be difficult to wean • Impractical as equipment required for its measurement is not available routinely in ICU • P 0.1 / MIP < 0.3 - a good early predictor of weaning success
Other Criteria… Pressure – time product • Integral of the difference between pleural pressure during assisted breathing and the recoil pressure of the chest during passive breathing • Measures work of breathing • Limitation – cumbersome measurements → not widely applied Tension time index • Product of transdiaphragmatic pressure during tidal breathing as a proportion of the maximal transdiaphragmatic pressure and the duration of inspiration • Accounts for isometric contraction • Correlates well with oxygen cost of breathing • Requires esophageal and gastric balloons → impractical
Other criteria… It is found to be a better predictor of weaning success than traditional parameters and RSBI Gastric intramucosal pH( pHi) • Periods of increased respiratory muscle activity are associated with decreased splanchnic blood flow and decrease in gastric mucosal pH • pHi estimated using gastric juice PCO2 before and during SBT → Gastric pHi > 7.30 or a change of <0.09 predicts successful extubation • Criticism → Gastric juice PCO2 is extremely unstable → unreliable measurement
Weaning Procedure • Rapid ventilator discontinuation • Spontaneous breathing trials • Pressure support ventilation (PSV) • SIMV • Other Modes used for weaning
Rapid ventilator discontinuation Sbts are superior to both SIMV and PS in both duration of weaning and likelihood of success after weaning • Considered in patients with no underlying cardiovascular, pulmonary, neurologic, or neuromuscular disorders and patients receiving ventilatory support for short periods e.g. post-op patients Patient on ventilator for < 72 hrs Good spont RR, MV, MIP, f/Vt SBT for 30 to 120 min. EXTUBATE if no other limiting factor
Spontaneous Breathing Trial • SBT can be in the form of T – tube trial or PSV of 5-10 cm H2O or CPAP 5-7 cmH2O • T-Tube trial: allows spontaneous breathing interspersed with periods of full ventilatory support • ADVANTAGES • Tests pt’s spontaneous breathing ability • Allows periods of work and rest • Weans faster than SIMV • DISADVANTAGES • Abrupt transition difficult for some pts • No alarms, unless attached to vent. • Requires careful observation.
A T-piece (or trach-collar) trial involves the patient breathing through a T-piece (essentially the endotracheal tube (ett) plus a flow of oxygen-air and no ventilatory assistance) for a set period of time. The work of breathing is higher than through a normal airway (although this simulates laryngeal edema/airway narrowing). If tolerated, the chances of successful extubation are high. If not reattachment to a ventilator is simple. Gas flow to inspiratory limb should be at least twice that of the patient’s spontaneous minute ventilation in order to meet the patient’s peak inspiratory flow rate. An extension piece of about 12 inches should be added to the expiratory limb to prevent entrainment of room air. T Tube Adapter
Weaning protocol for SBT with a T-Tube There is evidence that the detrimental effects of ventilatory muscle overload, if it is going to occur, often occur early in the SBT.73,108,110,128 Thus, the initial few minutes of an SBT should be monitored closely before a decision is made to continue (this is often referred to as the “screening” phase of an SBT). Thereafter, the patient should continue the trial for at least 30 min but for not 120 min102 to assure maximal sensitivity and safety. It also appears that whether the SBT is performed with low levels of CPAP (eg, 5 cm H2O), low levels of pressure support (eg, 5 to 7 cm H2O), or simply as “T-piece” breathing has little effect on outcome.101,129–131 CPAP, however, conceivably could enhance breath triggering in patients with significant auto-PEEP.132,133 Optimize the patient’s medical condition suction, adequate humidification, bronchodilator therapy, good nutrition, optimal position, psychological counseling, adequate staff, equipment, no sedatives Prepare for T-Tube trial 3 min. screening trial Measure TV,RR Measure MIP thrice selecting the best If signs of intolerance are present . Formal SBT for 30 – 120 min MIP < -20 cm H20 TV spon. > 5 ml/kg RR spon. < 35/min. Put the patient back on previous ventilator settings no signs of intolerance Repeat next trial after 24 hrs extubate
SBT with CPAP • CPAP circuit overcomes some of the work of breathing through the tracheal tube and prevents airway collapse. • CPAP may improve lung mechanics and reduce the effort required by mechanically ventilated patients with air flow obstruction and may enhance breath triggering in patients with significant auto-PEEP.
SBT with Pressure Support • Trachea can be extubated directly from PS as PS overcomes the tube resistance • 7cmH2O of pressure support is required to overcome the resistance through a size 7.5mm (internal diameter) endotracheal tube • 3cmH2O PS is required through a tracheostomy • If a smaller tube is in place, pressure support of 10 cmH2O is required.
Weaning with SIMV • Breaths are either spontaneous or mandatory • Mandatory breaths are synchronized with patient’s own efforts • ADVANTAGES • Gradual transition • Easy to use • Minimum MV guaranteed • Alarm system may be used • Should be used in comb. • with PSV/CPAP • DISADVANTAGES • Prolongs weaning • May worsen fatigue
Protocol of SIMVWeaning Monitor patient’s appearance , respiratory rate , SpO2, BP, obtain ABG sample Start with SIMV rate at 80% of full support f is then decreased by 2 – 4 breaths twice daily If deterioration → ↑ SIMV rate If the patient tolerates an SIMV rate of 2-4 breaths for> 2 hrs Allow pt’s resp msls to rest at night by ↑ing SIMV rate Consider extubation
Weaning with PSV Pressure support is given with each spontaneous breath to ensure an adequate TV • ADVANTAGES • Gradual transition • Prevents fatigue • Increased pt comfort • Weans faster than SIMV alone • Pt can control cycle length, rate • and inspiratory flow. • Overcomes resistive WOB d/t • ET tube and circuit. • DISADVANTAGES • ↑ed MAP versus T-Tube • TV not guaranteed
Protocol of PSV weaning PSV is adjusted to deliver TV 10-12 ml/kg, (PSVmax) Monitor patient’s appearance , respiratory rate , SpO2, BP, obtain ABG sample PSV level is decreased by 2-4 cm H2O twice daily to maintain TV If patient tolerates PSV level of 5-8 cm H2O for greater than 2 hrs Consider extubation
Weaning with SIMV +PSV • The addition of pressure support with SIMV can overcome the work of breathing during “spontaneous breaths” due to endotracheal and tracheostomy tubes, demand flow systems and ventilator circuits • The pressure support level needed to overcome the imposed work of breathing during IMV weaning can be estimated as • PSV = (PIP-Pplat) ×V max Vmech PIP =peak inspiratory pressure during a machine delivered breath Pplat = pateau pressure during a mechanical inspiratory volume hold Vmech = flow during a machine breath Vmax = patient’s spontaneous peak inspiratory flow
Weaning protocol for SIMV + PSV SIMV rate is set at 2 breaths/min lower than the rate given by A/C mode + PSV 15-20 cmH2O Reduce SIMV rate in steps of 1-3 breaths/min + PSV 15-20 cm H2O Monitor patient’s appearance , respiratory rate , SpO2, BP, obtain ABG sample When SIMV rate becomes 5 breaths/min, stop SIMV and continue with PSV 15-20 cm H2O Allow pt’s resp msls to rest at night by ↑ing SIMV rate Reduce PSV in steps of 2 cm H2O until PSV is 5-6 cmH2O Extubate the patient
Weaning : Selecting an Approach!!! • Many studies have compared the different methods of weaning • Common conclusions are • No clear superiority exists between T-tube weaning and pressure support based weaning • SIMV is the least efficient technique of weaning
Weaning : Selecting an Approach!!! To summarize, there are advantages and disadvantages to each of the weaning methods .however, the best appraoch may be the one with which the clinician is most familiar anf is based on a sound rationale …
Other Modes used for weaning • Non invasive ventilation (NIV) • Biphasic positive airway pressure (BiPAP) • Automatic tube compensation (ATC) • Volume support (VS) • Volume assured pressure support (VAPS) • Mandatory minute ventilation (MMV) • Servo controlled ventilation ( Automatic Ventilatory Support)
Non invasive Ventilation TECHNIQUE OF PROVIDING ventilation without the use of an artificial airway It is used successfully in patients with OSA, acute ventilatory failure or impending ventilatory failure Used to support ventilation without the use of an artificial airway Useful as a bridge to total withdrawal of ventilatory support Suggested Indications Alternative weaning technique for patients who failed conventional weaning sp COPD pts NIV as a prophylactic measure for patients with a high risk for reintubation NIV for the treatment of respiratory insufficiency after extubation (post-extubation failure)
For some subgroups (hypercapnic respiratory insufficiency, especially in COPD patients) NIV may be helpful in expediting the weaning process. However, its use cannot be recommended for all patients failing a SBT. Clear criteria for discontinuation of NIV must be defined. Positive effects of prophylactic NIV treatment in patients at risk for reintubation seem likely, but larger studies have yet to confirm this observation.
Volume support • The machine measures the delivered volumes and adjusts the pressure support to meet desired “goal” • Allows automatic weaning of P support as compliance alters. Preset & constant C = V P changes during weaning & guides P support level P support dependent on C compliance ↑ - P support ↓ ↓ - P support ↑ Deliver desired TV
Volume support… • Advantages • Provides a controlled tidal volume • Increases patient comfort • Helps in weaning or during awakening from anaesthesia
Volume assured pressure support We set the desired minimum tidal volume and pressure support level . Once a breath is triggered vent tries to achieve the desired tidal volume at the earliest by increasing the fflow . If the desired tidal volume equals the set tidal volume breath is considered as a pressure support breath if the delivered volume is less than the preset volume, the ventilator switches from a pressure limited breath to a volume limited breath..
Volume assured pressure support • Disadvantages • May prolong the inspiratory times leading to air trapping and undesirable cardiovascular effects • Advantages • Assures a stable tidal volume
Automatic tube compensation • Aventilatory method aimed at compensating for nonlinear pressure drop across the endotracheal tube during spontaneous breathing. • Overcomes the imposed work of breathing due to artificial airways. • Provides dynamic ventilatory support of each spontaneous breath by delivering the exact amount of pressure necessary to overcome the resistive load of the endotracheal tube for the flow measured at the time, so-called variable pressure support. • At least as successful as use of simple T-tube or low-level PS for weaning from mechanical ventilation.
Automatic tube compensation High circuit pressure Low carinal pressure Pressure drop across the circuit is the cause of WOB with an endotracheal tube ATC raises the carinal pressure and hence decreases the work of breathing ∆P (P support) α (L / r4) αflow αWOB