Download
1 / 55
1.35k likes | 5.92k Vues
WEANING FROM MECHANICAL VENTILATION. Dr MEGHA JAIN. University College of Medical Sciences & GTB Hospital, Delhi. HEADINGS. Purpose of weaning and extubation. Rationale of predictive indices in weaning. Application of weaning parameters. Methods of weaning. Impediments to weaning.

E N D
WEANING FROM MECHANICAL VENTILATION Dr MEGHA JAIN University College of Medical Sciences & GTB Hospital, Delhi
HEADINGS • Purpose of weaning and extubation. • Rationale of predictive indices in weaning. • Application of weaning parameters. • Methods of weaning. • Impediments to weaning. • Extubation and terminal weaning.
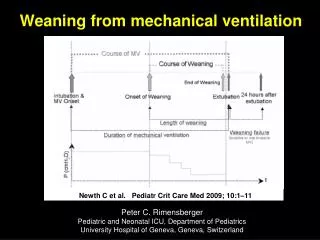
Different stages in mech. Ventilated pts. 1. Treatment of ARF 3. Assessing readiness to wean 5. Extubation 6. Reintubation 2. Suspicion 4. SBT Admit Discharge
DEFINITIONS • Weaning is the gradual reduction in the level of ventilatory support. • Weaning success: effective spontaneous breathing without any mechanical assisstance for 24 hrs or more. • Weaning failure: when pt is returned to mechanical ventilation after any length of weaning trial. • Signs of weaning failure: abnormal blood gases, diaphoresis, tachycardia, tachypnea, arrythmias, hypotension.
Morbidity Associated With Prolonged Intubation and Mechanical Ventilation • Vocal cord granulomas • Ulceration of the true vocal cords • Circumferential fibrous stenosis of trachea • Epithelial damage, loss of cilia, and impairment of tracheal mucus clearance • Risk factor for nosocomial pneumonia • Precludes oral feeding
The assessment of weaning proceeds in two phases: Phase 1: To ensure that certain basic criteria regarding initial reason for mechanical ventilation are satisfied Phase 2: Determine whether weaning is likely to succeed on the basis of specified criteria
READINESS FOR VENTILATOR WEANING Major determinants of ability to wean can be classified into three categories: • oxygenation • ventilatory pump function • neuropsychiatric status
OXGYGENATION • Criteria of Adequacy PaO2 > 60 mmHg on FIO2 <0.4 at minimal PEEP, PaO2/FIO2>200 • Selected causes of failure: • Hypoventilation: neurologic injury or drugs • V/Q mismatch: severe CHF • Anatomic (R-to-L) shunt (e.g. intracardiac, pulmonary A-V malformation).
VENTILATION • Criterion of Adequacy PaCO2 < 50 mmHg or within 8 mmHg of baseline • Selected causes of failure • respiratory drive: sedation, drug overdose. • resp bellows function: diaph weakness, N-m disease • CO2 production without compensatory ↑ in alveolar Ve: • fever, hypermetabolism, carbohydrate overfeeding - dead space ventilation without compensatory ↑ alveolar Ve: • PE, bullous emphysema
NEUROPSYCHIATRIC INTEGRITY • Criteria of adequacy Awake, alert, cooperative, with intact gag and swallowing • Selected causes of failure Cerebrovascular accident Sleep deprivation/ICU psychosis Drug therapy Depression Psychological dependency on ventilatory support
WEANING CRITERIA • Used to evaluate the readiness of a patient for weaning trial. • Common weaning criteria: Ventilatory criteria Oxygenation criteria Pulmonary reserve Pulmonary measurements Other factors
VENTILATORY CRITERIA • PaCO2: < 50 mmhg with pH >/= 7.35. • VC: > 10 to 15 ml/kg • Spontaneous VT: > 5 to 8 ml/kg • Spontaneous RR: < 30/min • Minute ventilation: < 10 lts PaCO2 – most reliable indicator VC and spon VT – indicate mechanical cond of lungs A high spon RR and MV indicate ↑ WOB
OXYGENATION CRITERIA • PaO2 without PEEP > 60 mmhg @FiO2 upto 0.4 • PaO2 with PEEP > 100 mmhg @ FiO2 upto 0.4 • SaO2 > 90% @ FiO2 upto 0.4 • Qs/Qt < 20% • P(A-a)O2 < 350 mmhg • PaO2/FiO2 > 200 mmhg Qs/Qt estimate wasted pulmonary perfusion P(A-a)O2 is related to degree of hypoxemia/shunt In pts with anemia or dysfunct Hb, PaO2 and SaO2 don’t reflect true oxygenation status So arterial oxygen content should be measured
PULMONARY RESERVE AND MEASUREMENTS • Pulmonary reserve: Max. voluntary ventilation – 2×min. vent@FiO2 upto 0.4 Max. Insp. Pressure < -20 to -30 cmH2O in 20 sec. • Pulmonary measurements: Static compliance > 30 ml/cm H2O Vd/Vt < 60% Pulmonary reserve requires active pt cooperation Pulmonary measurements indicate workload needed to support spont. ventilation
COMBINED WEANING INDICES • Simplified weaning index: evaluates efficiency of gas exchange. = ( fmv (PIP – PEEP)/MIP) × PaCO2/40. should be < 9/min. • CROP index: evaluates pulmonary gas exchange and balance b/w respiratory demands and respiratory neuromuscular reserve. = ( Cd × MIP × PaO2/PAO2)/f. Should be > 13 ml/breath/min. • RSBI: should be < 105 cycles/min/lt. = f/Vt. Most accurate test to predict weaning success.
RSBI • First described by Yang and Tobin in 1991. • It’s a one min. trial of unassisted breathing measured during the T –piece trial. • Main defect: excessive false +ves • Should not be measured until sedative and narcotic effects have adequately abated and the pt. triggers 2 to 3 breaths/min above ventilator set rate. • Measure RR and MV for 1 min. during unassisted breathing( 0 PEEP/5 cmH2O PSV). • At end of 1 min. divide MV by RR to calculate avg. tidal vol. • Divide RR by TV to obtain RSBI.
OTHER FACTORS • Metabolic factors: * Inadequate nutrition – protein catabolism * Overfeeding - ↑ CO2 production * Phosphate, ? Magnesium deficiency - ↓respi pump functn * Impaired O2 delivery - ↓respi pump functn. • Renal function: * Patient should have adeq renal output (> 1000 ml/day) * Monitor electolytes to ensure adequate respi msl functn • Cardiovascular function * Ensures sufficient O2 delivery to tissues *Cardiac rate, rhythm, BP, CO and CI should be optimal with minimal pressure support • CNS assessment * Assess for LOC, anxiety, dyspnea, motivation * CNS should be intact for protection of airway.
Weaning methods • Spontaneous breathing trial • SIMV with pressure support. • PSV • Rapid ventilator discontinuation: pt.on vent for < 72 hrs., has good spont RR, MV, MIP, f/Vt SBT for 30 to 120 min. EXTUBATE if no other limiting factor
Spontaneous Breathing Trial • T-Tube trial: allows spont. breathing several times per day interspersed with periods of ventilatory support. • Initial SBT’s may last only 5 to 30 min. • Resume mechanical ventilation at night or if distress occurs. ADVANTAGES Tests pt’s spon breathing ability Allows periods of work and rest Weans faster than SIMV DISADVANTAGES Abrupt transition difficult for sm pts No alarms, unless attached to vent. Requires careful observn.
Weaning protocol for a SBT with a T-Tube Verify that pt is a candidate for vent. discontinuation Primary cause reversed Pt is afebrile, awake, alert and free of seizures HD stable with adeq. Hb, S.E. Oxygenation and ventilation adequate PaO2>/= 60mmhg on FiO2 </= 0.4 with PEEP/CPAP </= 5 to 8 cmH2O PaO2/FiO2 > 150 to 200 mmhg PaCO2 < 50; pH > 7.35 Other indices: - f/VT < 105 - MIP < -20 cm H2O - f < 30 and > 6/min. - VC > 10 to 15 ml/kg - TV > 5 ml/kg
Weaning protocol for a SBT with a T-Tube Prepare for T-Tube trial Adequate staff, equipment, no sedatives 3 min. screening trial Measure TV,RR Measure MIP thrice selecting the best Formal SBT of upto 2 hrs. MIP < -20 cm H20 TV spon. > 5 ml/kg RR spon. < 35/min. Continue trial for 30 – 120 min. Extubate if no signs of intolerance
Signs of intolerance of SBT • Agitation, anxiety, diaphoresis or change in mental status • RR > 30 to 35/min • SpO2 < 90% • > 20% ↑ or ↓ in HR or HR > 120 to 140/min • SBP > 180 or < 90 mmhg. Such pts are returned to full ventilatory support for 24 hrs. to allow the ventilatory msls. to recover.
Weaning with SIMV • Involves gradual reduction in machine rate based on ABG and clinical assessment. • Rate is generally adjusted in increments of 2 breaths/min. followed by pt assessment. ADVANTAGES Gradual transition Easy to use Minimum MV guaranteed Alarm system may be used Should be used in comb. with PSV/CPAP DISADVANTAGES Pt. – ventilator asynchrony Prolonges weaning May worsen fatigue
Pressure Support Ventilation (PSV) Patient determines RR, VE, inspiratory time – a purely spontaneous mode • Parameters • Triggered by pt’s own breath • Limited by pressure • Affects inspiration only • Uses • Complement volume-cycled modes (i.e., SIMV) • Does not augment TV but overcomes resistance created by ventilator tubing • PSV alone • Used alone for recovering intubated pts who are not quite ready for extubation • Augments inflation volumes. PSV is most often used together with other volume-cycled modes. PSV provides sufficient pressure to overcome the resistance of the ventilator tubing, and acts during inspiration only.
Pressure support ventilation • Begin with PSV that achieves a RR of 20 to 25/min or less. • Adjust pressure to achieve a TV of 8 to 10 ml/kg. • Reduce PSV 2 to 4 cm H2O as tolerated, ideally at least twice daily. • Consider extubation when pt. tolerates PSV of 5 to 8 cm H2O for 2 hrs with no apparent distress.
Pressure support ventilation ADVANTAGES Gradual transition Prevents fatigue Increased pt comfort Weans faster than SIMV alone Every breath is supported Pt can control cycle length, rate and inspiratory flow. Overcomes resistive WOB d/t ET tube and circuit. DISADVANTAGES Large changes in MV can occur ↑ed MAP versus T-Tube TV not guaranteed
Mandatory minute ventilation • Also called minimum minute ventilation, provides predetermined minute ventilation when pt’s spon. breathing effort becomes inadequate. • Prevents hypoventilation and respi. acidosis in final stages of weaning. • Trigger is ↑ in mandatory RR when actual MV < preset MV. • All mandatory breaths are volume cycled. • Desired min. minute vol. is preset on the vent. Slightly lesser than that required to normalize PaCO2. • If distress + pt tends to ↑ RR at expense of ↓ TV , leads to significant dead space ventilation
Mandatory minute ventilation ADVANTAGES Backup ventilation ensured, Potential to speed weaning compared with SIMV. DISADVANTAGES May not ensure efficient pattern of breathing, Rapid shallow breathing possible with MMV.
Automatic Tube Compensation ∆P (P support) α (L / r4) α flow α WOB • Compensates for the resistance of ETT • Facilitates “ electronic weaning “ i.e pt during ATC mimic their breathing pattern as if extubated ( provided upper airway contorl provided) • OPERATION As the flow ↑ / ETT dia ↓, the P support needs to be ↑to ↓WOB
Feed resistive coef of ETT • Feed % compensation desired • Measures • instantaneous flow Calculates P support proportional to resistance throughout respiratory cycle Limitation – resistive coef changes in vivo ( kinks, temp molding, secretions) Under/ overcompensation may result. Static condition – single P support level can eliminate ETT resistance Dynamic condition – variable flow e.g. tachypnoea & in diff phases of resp. - P support needs to be continously altered to eliminate dynamically changing WOB d/t ETT
Proportional Assist Ventilation • Targets fixed portion of patient’s workduring “spontaneous” breaths • Automatically adjusts flow, volume and pressure needed each breath
ELASTANCE (TV) RESISTANCE (Flow) WOB Ventilator measures – elastance & resistance Clinician sets -“Vol. assist %” reduces work of elastance “Flow assist%” reduces work of resistance's Increased patient effort (WOB) causes increased applied pressure (and flow & volume)
Limitations 1. Elastance (E) & resistance (R) cannot be measured accurately. 2. E & R vary frequently esp in ICU patients. 3. Curves to measure E ( PV curve) & R(P-F curve ) are not linear as assumed by ventilator.
Noninvasive • ventilation without artificial airway • Nasal , face mask • adv. • Avoid intubation / c/c • Preserve natural airway defences • Comfort • Speech/ swallowing + • Less sedation needed • Intermittent use • Disadv • Cooperation • Mask discomfort • Air leaks • Facial ulcers, eye irritation, dry nose • Aerophagia • Limited P support • e.g. BiPAP, CPAP
Role of tracheostomy in weaning • Performed in ventilator dependent pts., timing is controversial. • Beneficial in: ↓ed sedation requirement, articulated speech, allowed orally, enhanced mobility.
Role of tracheostomy in weaning • Early tracheostomy ( in 2 days of admission ) reduces mortality, risk of pneumonia, accidental extubation, ICU length of stay. Reduces dead space Less airway resistance ↓ed WOB Better suctioning Improved pt comfort Facilitates weaning
Complications • Misplacement • Hemorrhage • Obstruction • Displacement • Impairment of swallowing reflexes • Late tracheal stenosis.
Weaning failure • Defined as when pt is returned to mech. Ventilation after any length of weaning trial or is reintubated within 48 hrs following extubation. • Causes: 1. ↑ed air flow resistance- ET tube, abdominal distention, tracheal obstruction. 2. ↓ed compliance- atelectasis, ARDS, tension pneumothorax, obesity, retained secretions, bronchospasm, kinking of ETtube. 3. Electrolyte imbalance, inadequate nutrition.
Indicators of weaning failure • Blood gases- ↑ing PaCO2 ( >50 mmhg) ↓ing pH < 7.30 ↓ing PaO2 (<60 mmhg) ↓ing SpO2 (<90%) ↓ing PaO2/FiO2 (<150 mmhg) • Vital signs- ↑ing HR ( by > 20/min. or > 110/min.) abnormal ECG changing BP ( 20 mmhg SBP or 10 mmhg DBP)
Indicators of weaning failure • Respiratory parameters: ↓ing TV ( < 250 ml) ↑ing RR ( > 30/min) ↑ing f/TV ratio ( > 105 cycles/L) ↓ing MIP ( < -20 cm H2O) ↓ing static compliance ( < 30 ml/cm H2O) ↑ing VD/VT ( > 60%)
Pathophysiology of weaning failure • NONRESPIRATORY PARAMETERS AFFECTING ABILITY TO WEAN Nutritional status Fluid balance Metabolic and acid-base derangements Cardiac Function Renal function Neuropsychiatric factors
Nutritional status Malnutrition has adverse effects on the respiratory system • ↓respiratory muscle strength and function • ↓diaphragmatic mass and contractility • ↓endurance
Nutritional status Overnutrition may impede weaning • High CO2 Produced by excessive CHO loading • Other causes of increased CO2 production: fever, sepsis, shivering, seizures, and inefficient ventilation due to dead space, PE
Metabolic abnormalities • Hypophosphatemia • Hypocalcemia • Hypothyroidism
Sleep Deprivation and Psychological Issues • Twilight awareness -> nap during the day -> shift day-night cycle • Give sedative-hypnotic at bedtime to restore normal daily cycle • Depression in the long-term ICU patient: • TCA at bedtime for sedative effect and to forestall depression. • Anxiety • Adequate sedation: only to minimize detrimental WOB • Very slow changes in PS level: to prevent anxiety induced by sudden changes to the response of the lung stretch receptors
Ventilator induced diaphragmatic dysfunction • VIDD – loss of diaphragmatic force generating capacity related to use of mech. Ventilation can ocurr as early as 12 hrs. and reduction in max force production is of the order of 30 – 50 % after 1 – 3 days of CMV. • Causes of VIDD – msl. atrophy, oxidative stress, structural injury, msl fiber remodelling. • Management - * Minimise use of NM blockers, steroids * Optimize PO4, Mg, nutrition. * Cervical magnetic stimulation of phrenic nerve * Antioxidant supplementation.
Critical care illness neuromyopathy • Causes – sepsis, malnutrition, paralysing agents, sedatives, narcotics, steroids. • Affects all msls. Including diaphragm and intercostals. • B/L proximal msl weakness. • Diagnosis using Medical Research Council Score( < 48), electrophysiological testing and msl biopsy if appropriate. • Transdiaphragmatic pressure in response to B/L phrenic nerve stimulation. • Treatment options * Good nutrition * Withdrawal of offending drugs * Inspiratory msl exercises
Prolonged mechanical ventilation • Required in 3 to 7 % of ventilated pts. • Unless cause is irreversible ( high spinal cord injury) pt should not be considered permanently ventilator dependent until 3 mths of weaning attempts have failed. • Often transferred to regional weaning centers/long term care facilities. • Goal is to restore pt to highest level of independent function possible.
Complications of PMV • Infection • Bacterial Pneumonia • Line sepsis • Volume Overload • Laryngeal Edema • Pneumothorax • Tracheal Bleeding • Ileus • DVT • Additional Complications if Tracheostomy is necessary
Extubation • Discontinuation of invasive PPV involves 2 steps: * separation of pt. from vent. based on assessment of * removal of artificial airway. airway patency & protection Parameters for airway patency Cuff leak test Qualitative Quantitative audible air leak< 110 ml air leak Parameters for airway protection Effective cough Secretion volume Mental status