Weaning from mechanical ventilation
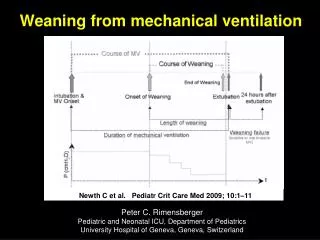
Newth C et al. Pediatr Crit Care Med 2009; 10:1–11. Weaning from mechanical ventilation. Peter C. Rimensberger Pediatric and Neonatal ICU, Department of Pediatrics University Hospital of Geneva, Geneva, Switzerland. Reported extubation failure rates in PICUs range from 4.1% to 19%.

Weaning from mechanical ventilation
E N D
Presentation Transcript
Newth C et al. Pediatr Crit Care Med 2009; 10:1–11 Weaning from mechanical ventilation Peter C. Rimensberger Pediatric and Neonatal ICU, Department of Pediatrics University Hospital of Geneva, Geneva, Switzerland
Reported extubation failure rates in PICUs range from 4.1% to 19% Baisch SD, Wheeler WB, Kurachek SC, Cornfield DN. Extubation failure in pediatric intensive care incidence and outcomes. Pediatr Crit Care Med 2005; 6:312–318. Edmunds S, Weiss I, Harrison R. Extubation failure in a large pediatric ICU population. Chest 2001; 119:897–900. Fontela PS, Piva JP, Garcia PC, et al. Risk factors for extubation failure inmechanically ventilated pediatric patients. Pediatr Crit Care Med 2005; 6166–170. Weaning / Extubation failure: Is it a real problem in the PICU ?
Effect of Mechanical Ventilator Weaning Protocols on Respiratory Outcomes in Infants and Children: A Randomized Controlled Trial In contrast with adult patients, the majority of children are weaned from mechanical ventilator support in 2 days or less. Weaning protocols did not significantly shorten this brief duration of weaning. Adrienne G. Randolph et al. JAMA 2002;288(20):2561-2568
Weaning: The key questions • Is the cause of respiratory failure gone or getting better ? • Is the patient well oxygenated and ventilated ? • Can the heart tolerate the increased work of breathing ?
Discontinuation of Mechanical Ventilation To discontinue mechanical ventilation requires: • Patient preparation • Assessment of readiness • For independent breathing • For extubation • A brief trial of minimally assisted breathing • An assessment of probable upper airway patency after extubation • Either abrupt or gradual withdrawal of positive pressure, depending on the patient’s readiness
Factors that may contribute to extubation failure in pediatric patients • young age • duration of mechanical ventilation • prolonged treatment with sedatives and analgesics Fontela PS, Piva JP, Garcia PC, et al. Risk factors for extubation failure in mechanically ventilated pediatric patients. Pediatr Crit Care Med 2005; 6166–170.
Failure rate of planned extubations of patients within the first 48 hrs of arrival in the pediatric intensive care unit (PICU) is, on average, half that of the rate for patients ventilated for longer than 48 hrs. Kurachek SC et al.Crit Care Med 2003; 31:2657–2664
Ventilation > 48 hours: contrary to common perception there is no relationship between the duration of MV and rates of failed extubation Kurachek SC et al.Crit Care Med 2003; 31:2657–2664
Classical Methods for Gradually Withdrawing Ventilator Support
The most common weaning approach: gradual reduction of ventilatory support 1) By reducing ventilatroy rate: IMV or SIMV 2) By reducing inspiratory pressure: PS PS is often combined with IMV/SIMV during weaning Volume support and volume-assured pressure support are special forms of PS available in certain ventilators that guarantee a minimal tidal volume per assisted breath. Weaning with volume support is semiautomatic, where the PS level required to maintain a certain tidal volume is reduced automatically as respiratory mechanics improve.
Getting ready for extubation • Weaning • decrease the PEEP (4-5) • decrease the rate • decrease the PIP (as needed) • What you want to do is decrease what the vent does and see if the patient can make up the difference….
Controlled ventilation Ventilator work Paw = Pvent + Pmus Trigger patient Inspiration Expiration Airway pressure Assisted Ventilation Pvent Patient work Ventilator work J.J. Marini, et al Am Rev Respir Dis 1986: 134: 902-909
Spontaneous Breathing Trials and Extubation Readiness Tests
Of the 323 patients (77%) who passed the SBT and were extubated, 14% were reintubated within 48 hrs. Respiratory rate, tidal volume, rapid shallow breathing index (RSBI), and maximal negative inspiratory pressure (PImax) were all poor predictors of extubation outcome. Farias JA et al. Intensive Care Med 2002; 28:752–757 Spontanoeus Breathing Test (SBT) SBT conducted on PS of 10 cm H2O versus SBT using a T-piece no difference Farias JA et al. Intensive Care Med 2001; 27:1649–1654
Rapid Shallow Breathing Index (RSBI): f/VT The frequency to tidal volume ratio (or rapid shallow breathing index, RSBI) is a simple and useful integrative indicator of the balance between power supply and power demand. In adults: A rapid shallow breathing index < 100 generally indicates adequate power reserve. In this instance, the RSBI indicated that spontaneous breathing without pressure support was nottolerable, likely due in part to the development of gas trapping.
Limitations of RSBI in children wide range of age groups with different respiratory rates
Weaning failure: Objective Criteria RR above normal age limits: < 6 months: 20–60 breaths/min < 2 years: 15–45 breaths/min < 5 years: 10–35 breaths/min or > 1,5 x normal F. Leclerc, O. Noizet, W. Chaari, A. Sadik, Y. Riou Principles of mechanical ventilation weaning in paediatric intensive care Annales Françaises d’Anestésie et de Réanimation 28 (2009) 685–687
Rapid Shallow Breathing Index (RSBI): f/VT Compliance, Resistance, Oxygenation, Pressure Index (CROP Index): (DynamicCompliance x Maximal Negative Inspiratory Pressure x (PaO2/PAO2)/ Respiratory Rate)
Rapid Shallow Breathing Index (RSBI): f/VT Compliance, Resistance, Oxygenation, Pressure Index (CROP Index): (DynamicCompliance x Maximal Negative Inspiratory Pressure x (PaO2/PAO2)/ Respiratory Rate) Volumetric Capnography: physiologic dead space (VD/VT)
Measurement of End-tidal CO2 and Dead Space The Single Breath CO2 Curve Phase 1: - airway deadspace Phase 2: - mixing of airway deadspace and alveolar gas Phase 3: - alveolar volume
The Single Breath CO2 Curve with added PaCO2 value Area X = volume of CO2 Area Y = wasted ventilation due to alveolar deadspace Area Z = wasted ventilation due to airway deadspace Physiologic VD / VT = (Y+Z) / (X+Y+Z) Physiologic Deadspace = (VD / VT) * (VT) Alveolar Deadspace = VD phys - VD airway
Deadspace to tidal volume ratio predicts successful extubation in infants and children VD/VT ≤ 0.50 reliably predicts extubation success with 75% sensitivity and 92% specificity, whereas a VD/VT > 0.65 identified patients at risk for failure Hubble CL, Gentile MA, Tripp DS, et al: Crit Care Med 2000; 28:2034–2040
The Single Breath CO2 Curve and VCO2 Airway deadspace (VD airway) = area p Volume of CO2 = area X. Adding volumes of each breath gives CO2 elimination in ml / min
Volumetric CO2 recording MV SV not present VCO2 Not ready to extubate
Volumetric CO2 Monitoring • Watch VCO2 (CO2 elimination) over time as wean ventilator • If mechanical ventilation taken over by spontaneous ventilation with VCO2 remaining stable or increasing, then probably approaching extubation point
Predictors of extubation success and failure in mechanically ventilated infants and children Khan, Nadeem; Brown, Andrew; Venkataraman, Shekhar T. Critical Care Medicine 199624(9):1568-1579
Predictors of extubation success and failure in mechanically ventilated infants and children Venkataraman ST Crit Care Med 2000; 28:2991–2996
Reasons for reintubation Venkataraman ST et al. Crit Care Med 2000; 28:2991–2996
Preextubation variables easily obtained at the bedside can predict the relative risk of reintubation a spontaneous tidal volume that is at least normal, a low FIO2, a low Paw, a low OI, a low PIP, a high dynamic compliance, a low FrVe (fraction of total minute ventilation provided by the ventilator) a normal or high Vt/Ti (mean inspiratory flow) are associated with a low risk of failure Venkataraman ST et al. Crit Care Med 2000; 28:2991–2996
Sedation? Adrienne G. Randolph et al. JAMA 2002;288(20):2561-2568
The “air leak” testto predict which patients are at risk for postextubation stridor and extubation failure 76% of the physicians routinely use the “air leak” test test prior to extubation Foland JA, Super DM, Dahdah NS, Mhanna MJ. The use of the air leak test and corticosteroids in intubated children: a survey of pediatric critical care fellowship directors. Respir Care 2002; 47:662–666
The ‘air leak’ testto predict which patients are at risk for postextubation stridor and extubation failure Increased risk for post-extubation stridor or extubation failure when there is absence of a leak around the ETT or leak at a > 30 cm H2O Kemper KJ et al. Crit Care Med 1991; 19:352–355 Seid AB et al. Arch Otolaryngol Head Neck Surg 1991; 117:880–882 A leak around the ETT at > 20 cm H2O had a sensitivity of 83.3% in predicting post-extubation stridor in patients age > 6 years Mhanna MJ et al. Crit Care Med 2002; 30:2639–2643 3 x higher incidence of adverse events in patients without an air leak at 25cmH2O Suominen Pet al. Paediatr Anaesth 2006; 16:641–647.
Prophylactic systemic corticosteroids in an attempt to minimize post-extubation stridor ? Reduced incidence of post-extubation stridor in both neonatal and pediatric patients Trend towards decreased rates of re-intubation in the corticosteroid groups (statistically not significant) But there was considerable variation noted in the pediatric trials examined in this meta-analysis, which the authors attributed to possible differences in risk among the populations studied. Markovitz BP, Randolph AG. Corticosteroids for the prevention of reintubation and postextubation stridor in pediatric patients: A meta analysis. Pediatr Crit Care Med 2002; 3:223–226.
Prophylactic systemic corticosteroids in an attempt to minimize post-extubation stridor ? In neonates: RR 0.42; 95% CI 0.07 to 2.32 In children: significantly reduced in children with underlying airway abnormalities (n = 62) but not in the study that excluded these children (n = 153) In adults RR 0.48; 95% CI 0.19 to 1.22 for reintubation (n = 1953) RR 0.47; 95% CI 0.22 to 0.99 for stridor Markovitz BP, Randolph AG, Khemani RG: Corticosteroids for the prevention and treatment of post-extubation stridor in neonates, children and adults. Cochrane Database Syst Rev 2008; (2):CD001000
Using corticosteroids to prevent (or treat) stridor after extubation has not proven effective for neonates, children or adults. However, given the consistent trend toward benefit, this intervention does merit further study Markovitz BP, Randolph AG, Khemani RG: Corticosteroids for the prevention and treatment of post-extubation stridor in neonates, children and adults. Cochrane Database Syst Rev 2008; (2):CD001000
Extubation Criteria • Neurologic • Cardiovascular • Pulmonary
Neurologic • Patient must be able to protect his airway, e.g, have cough, gag, and swallow reflexes. • Level of sedation should be low enough that the patient doesn’t become apneic once the ETT is removed. • No apnea on the ventilator. • Must be strong enough to generate a spontaneous TV of 5-7ml/kg on 5-10 cm H2O PS or have a negative inspiratory force (NIF) of 25cm H2O or higher. • Being able to follow commands is preferred.
Cardiovascular • Patient must be able to increase cardiac output to meet demands of work of breathing. • Patient should have evidence of adequate cardiac output without being on significant inotropic support. • Patient must be hemodynamically stable.
Pulmonary • Patient should have a patent airway. • Pulmonary compliance and resistance should be near normal. • Patient should have “normal” blood gas and work-of-breathing on the following settings: • FiO2 <40% • PEEP ±5cm H2O • PS 5-8cm H2O • Spontaneous TV of 5-7ml/kg • Close to normal breath rate according to age
Conclusions:Weaning Readiness and Extubation Criteria • Ability to protect upper airway Effective cough Alertness • Improving clinical condition • Adequate lumen of trachea and larynx “Leak test” during airway pressurization
Conclusions:Weaning Readiness and Extubation Criteria Upper airway obstruction is the single most common cause of extubation failure. A reliable method of assessing readiness for weaning and predicting extubation success is not evident from the pediatric literature. Weaning is often not considered early enough in the course of ventilation.
Extubation • Control of airway reflexes • Patent upper airway (air leak around tube?) • Minimal oxygen requirement • Minimize pressure support (0 - max 10) (Normal compliance = Vt 8 ml/kg with PS of 8) • Comfortable spontaneous breathing • “Awake ” patient