Download
1 / 26
260 likes | 280 Vues
This article explores the role of growth hormone (GH) in human growth and development. It discusses the regulation of GH secretion by the hypothalamus and the effects of GH on various target tissues such as muscle, liver, and fat. The article also examines the indirect effects of GH through insulin-like growth factors (IGFs) and explains the net effects of GH on adipose tissue, liver, and muscle. Additionally, the article briefly mentions gigantism, acromegaly, and other pituitary cell types.

E N D
ANPS Anatomy & Physiology Endocrinology II
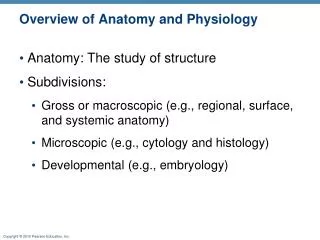
Gonadotrophs (LH / FSH cells) Corticotrophs (ACTH) Lactotrophs (PRL) Thyrotrophs (TSH) Somatotrophs (GH) Liver, Muscle, fat Hypothalamus GHRH GH releasing hormone GIH (somatostatin) GH inhibitory hormone CRH corticotropin releasing hormone TRH thyrotropin releasing hormone GnRH gonadotropin releasing hormone PRL prolactin releasing hormone Anterior pituitary cell types Adrenal gland Thyroid gland Ovary, Testis Mammary tissue
Somatotrophs Muscle, Liver, Fat (adipose), Bone (indirect) Growth Hormone (GH): primary hormone in human growth Hypothalamus GHRH GH releasing hormone GIH (somatostatin) GH inhibitory hormone • secreted throughout life but declines with age • produced by anterior pituitary somatotroph cells • targets muscle, liver and adipose (fat) tissues • GH has direct and indirect effects • indirect effects mediated by liver • insulin-like growth factors (IGFs) actions on • organs/bones • stimulated by hypothalamic GHRH release into portal • system • inhibited by somatostatin (GIH) and feedback • mechanisms GHRH • stimulates linear growth • increases organ growth, • increases muscle mass • generates fuel • stimulates lipolysis (decreases fat depots) • increases liver glucose production • decreases tissue glucose storage proliferation/survival effects (GH)
G protein coupled receptors GH release Hypothalamus GHRH (+) (GIH) Somatostatin (-) Anterior pituitarysomatotrophs GH Target tissues (muscle, liver, fat)
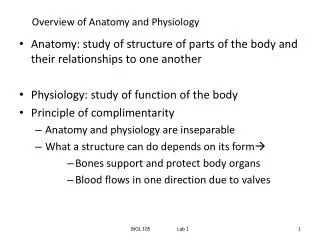
(IGF receptors) Insulin-like growth factors (IGFs) Somatic cell growth (IGF receptors) Bone chondrocyte/osteoblast function (IGF receptors) Hypothalamus GHRH (+) Somatostatin (-) (GPCR) Anterior pituitary GH Adipose tissue (GH receptors) Liver (GH receptors) Muscle (GH receptors)
(-) (-) IGFs IGFs Somatic cell growth organ/tissue size and function Bone chondrocyte/osteoblast function linear growth Hypothalamus GHRH (+) Somatostatin (-) Anterior pituitary GH Adipose tissue Lipolysis glucose uptake Liver Gluconeogenesis Muscle Amino acid uptake protein synthesis glucose uptake blood glucose free fatty acids lean body mass
Growth Hormone: net effects • Direct effects: • Adipose tissue • stimulates lipolysis, increasing blood free fatty acid fuel (muscle) • decreases glucose uptake • Liver • increases gluconeogenesis • increases IGF production (see indirect effects below) • Muscle • stimulates amino acid uptake/protein synthesis, increasing lean body mass • decreases glucose uptake (net effect of glucose on all 3 tissues is increased • blood glucose levels fuel for brain and other tissues) • Indirect effects (from IGF signaling): • increase organ size and function (increased cell survival/proliferation/differentiation) • stimulate bone chondrocyte function at epiphyseal plates to enhance linear growth • increase in lean muscle mass may be predominantly an IGF effect
Gonadotrophs (LH / FSH cells) Corticotrophs (ACTH) Lactotrophs (PRL) Thyrotrophs (TSH) Somatotrophs (GH) Liver, Muscle, fat Hypothalamus GHRH GH releasing hormone GIH (somatostatin) GH inhibitory hormone CRH corticotropin releasing hormone TRH thyrotropin releasing hormone GnRH gonadotropin releasing hormone PRL prolactin releasing hormone Anterior pituitary cell types Adrenal gland Thyroid gland Ovary, Testis Mammary tissue
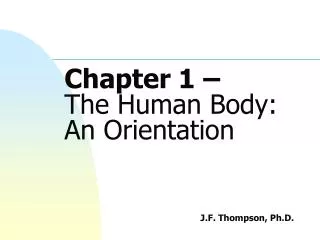
colloid follicular cells Thyroid follicle structure:
Thyroid stimulating hormone (TSH): Hypothalamus (TRH) • regulated by hypothalamic TRH • (thyrotropin releasing hormone) • TRH binds thyrotroph GPCRs for TSH release • TSH binds thyroid cells GPCRs for T3/T4 synthesis/release • T3/T4 bind to cytosolic receptors in target cells Ant. pituitary thyrotrophs TSH • Thyroid hormones: • regulates basal metabolic rate (BMR) • key in bone and nervous system development • increases gut carbohydrate absorption • decreases circulating cholesterol • stimulates lipolysis • increased protein breakdown (resulting in weight loss • if food is not increased) • facilitates autonomic function; • inotropic and chronotropic Thyroid follicular cells Thyroid hormone thyroxine/triiodothyronine (T4/T3)
colloid follicular cells Thyroid follicle structure:
Thyroid hormone (T3/T4) biosynthesis: • dietary iodide and thyroglobulin (TG) are • key substrates for T3/T4 synthesis • synthesis occurs on TG backbone in colloid • final T3/T4 products formed in cells • T3 is 4x more active; T4 is 20x more abundant • T4 is converted to T3 by deiodinases in tissues • Long T3/T4 feedback to pituitary/hypothalamus colloid
Cellular effects Physiological functions • Cellular effects: • consume more O2, burn more fuel, calorigenic • increase BMR (energy prod/unit time (cal)) • “make things work – better” • Physiological effects: • contributes to bone, nervous system, tissue • growth and development • increase ventilation, cardiac output, renal function • increase BMR – need more fuel; increase food intake, • increase lipolysis (decrease fat – release FFA), • increase carbohydrate absorption from gut; • decrease muscle mass is food not increased.
Thyroid Stimulating Hormone (TSH)
Hyperthyroidism (too much thyroid hormone): • people are “hyper”, BMR 10 – 100% above normal • nervousness, fine tremor at fingers • weightloss, hyperphagia • increase pulse pressure, heat intolerant, sweating • Grave’s disease – autoimmune antibodies activate TSH receptors resulting • in increased T3/T4 production (low circulating TSH) • treatment – radioactive iodine, propythiouracil (PTU), surgery • Hypothyroidism (too little thyroid hormone): • BMR falls to 40% of normal • “can’t think”, poor memory • lethargic, listless • skin dry, poor cold tolerance • Hashimoto’s disease – autoimmune antibodies destroy thyroid gland • (high levels of circulating TSH in blood) • hypothyroid children develop poorly (dwarfed) and can show mental • retardation (cretinism– rare) • treatment – thyroid hormone supplements
Parathyroid glands Calcium homeostasis • Calcium importance: • bone maintenance • nervous system signaling • muscle contraction, skeletal, smooth, cardiac • blood clotting • others....... • Three regulators: • parathyroid hormone (PTH) • vitamin D • calcitonin • Three integrated sites of action: • bone – largest reservoir of body calcium • GI calcium absorption • kidney calcium excretion
Parathyroid hormone (PTH) • produced by parathyroid gland • activates G protein coupled receptors on target tissues (bone, kidney) • Vitamin D • not one but class of compounds • synthesis in 3 tissues (skin, liver, kidney) • PTH important in final synthesis of active vit. D in kidney Skin Liver = calcidiol Kidney PTH hv Active form 1,25-(OH)2D = calcitriol
Body calcium homeostasis • free (ionized) calcium is active (50% free - 50% bound) • PTH and blood calcium levels are tightly balanced • drop in blood calcium leads to increased PTH release • via G protein coupled Ca sensing receptors in gland • PTH does 3 things: • PTH increases bone release of free calcium (slow) • PTH increases recovery of calcium from kidney (fast) • PTH stimulates kidney calcitriol (1,25-(OH)2D) synthesis • Calcitriol binds to steroid-type receptors in gut • to stimulate calcium absorption from food
25(OH)D = calcidiol 1,25(OH)2D = calcitriol *(active)
Calcitonin • peptide produced by thyroid C cells • decreases blood calcium; opposite effects of PTH and vit. D • blood calcium so tightly coupled with PTH/vit.D that • calcitonin is more important during development than in adults
Gonadotrophs (LH / FSH cells) Corticotrophs Lactotrophs Thyrotrophs Somatotrophs Hypothalamus GHRH GH releasing hormone GIH (somatostatin) GH inhibitory hormone CRH corticotropin releasing hormone TRH thyrotropin releasing hormone GnRH gonadotropin releasing hormone PRL prolactin releasing hormone Anterior pituitary cell types Adrenal gland Thyroid gland Ovary, Testis Liver, Muscle, fat Mammary tissue