The SHOULDER
The SHOULDER. THE SHOULDER. Anatomy Separations Fractured Clavicle Dislocations Supraspinatus Tendonitis. THE SHOULDER. Scapulothoracic Acromioclavicular Sternoclavicular Glenohumeral. Shoulder (Anterior View). Acromioclavicular Separation. Mechanisms of Injury:


The SHOULDER
E N D
Presentation Transcript
THE SHOULDER • Anatomy • Separations • Fractured Clavicle • Dislocations • Supraspinatus Tendonitis
THE SHOULDER • Scapulothoracic • Acromioclavicular • Sternoclavicular • Glenohumeral
Acromioclavicular Separation Mechanisms of Injury: Fall on the tip of the unprotected shoulder. Fall on the outstretched hand. Downward force on the acromion from above.
Grade of Injury of A/C Grade 1: Small tear of the capsule of the AC joint. No instability of joint. P.O.P.
Grade 2: Tear of the A/C joint capsule and a small tear of the coraco-clavicular ligaments.
Degree of Injury of A/C Grade 3: Tear of the acromio-clavicular ligament and the coraco-clavicular ligament.
Distal End of Clavicle GRADE 3 A-C SEPARATION
INSTABILITY OF A-C Jt. Grade 1: No instability of acromio-clavicular joint. Grade 2: Slight instability of A-C joint. ‘Springy’ clavicle. Grade 3: Total separation of A-C joint. The clavicle goes superiorly.
ACTIVE MOVEMENTS TO ASSESS A-C Jt. • Abduction • Cross Flexion
Active Abduction of the Shoulder Joint Grade 1: Full R.O.M. with pain at end of range. Grade 2: Has over 45º of motion but not 90º. Grade 3: less than 45º.
Return Time Estimates Grade 1: One week to ten days. Grade 2: Two to three weeks. Grade 3: Four to six weeks.
CRITERIA FOR RETURN Medical clearance. Full Range of Motion. Strength with 90% Able to do “high five” Protect the joint.
CLAVICLE • ‘S’ shape bone. • Protects neuro-vascular bundle and for muscle attachment. • Securely anchored at either end.
CLAVICLE FRACTURE Any force that brings the shoulder to the midline of the body. Direct impact to clavicle from superior or anterior direction.
Clavicle Fracture: Signs & Symptoms Pain and loss of function of shoulder. Spasm of trapezius and SCM (sternocliedomastoid) m. Arm held to body, shoulder elevated.
Clavicle Fracture: Signs & Symptoms May be palpable deformity when palpating the clavicle. In a pre-pubescent person, they may get a ‘greenstick’ fracture. MEDICAL REFERRAL!
Sternoclavicular Joint Costoclavicular Ligament Sternocavicular Ligament Clavicle 1st Rib Sternum
STERNOCLAVICULAR JOINT SEPARATION Very stable joint. Major ligaments are the sternoclavicular and costo-clavicular ligaments. Mechanism of Injury is the same as for the A.C. joint. Pain. Loss of motion. The unaffected side looks higher.
Flexion CW Rotation CCW Rotation Adduction Abduction Extension
ANATOMICAL PREDISPOSITION TO DISLOCATION • Glenoid Defects • Labral Defects • Neuromuscular Disorders
TERMINOLOGY LUX = DISLOCATE SUBLUX = PARTIAL DISLOCATION
TRAUMATIC Single force applies excessive overload to the soft tissues of the joint and often damages the Glenoid Labrum (Bankart Lesion) and the joint capsule.
ATRAUMATIC Athlete who has multiple joint laxities, who had frequent episodes of sub-luxations before and a relatively minor one results in dislocation. (Congenital hypermobility and/or muscle weakness)
ACQUIRED Sports such as swimming, gymnastics and baseball where repetitive micro-trauma, poor stretching and motion lead to capsular stretching. Eventual feeling of instability.
Bones of Shoulder Joint Clavicle Acromion Process Glenoid Posterior Anterior
LABRUM Cartilage ring around the glenoid. Deepens the socket of the G-H Joint.
Coracoclavicular Acromioclavicular Coraco-acromial Lig. Superior, Middle and Inferior Glenohumeral Ligament
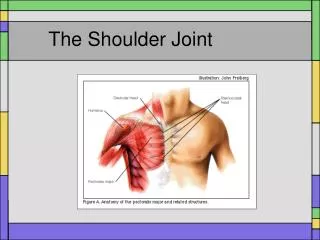
Pectoralis Major Deltoid Long Head of Biceps
1 2 3 4 • Subscapularis • Supraspinatus • Infraspinatus • Teres Minor
Posterior Musculature Supraspinatus Infraspinatus Teres Minor
PRIMARY MOVERS Deltoid Pectoralis Major (Latissimus Dorsi is posterior)
TYPES OF DISLOCATIONS Anterior (85%) Inferior (5%) Posterior (10%) Subcoracoid Dislocation
ANTERIOR DISLOCATION Arm in abduction and external rotation. Force is taken on the hand or arm which increases the external rotation of the arm causing the head of the humerus to dislocate.
INFERIOR DISLOCATION Arm is in excessive abduction and a force is taken on the hand pushing the head of the humerus inferiorly out of the glenoid.
Subcoracoid Dislocation The elbow is held away from the side and the hand can not turn onto the stomach.
POSTERIOR DISLOCATION The arm is in flexion and adduction. Force is taken on the hand, causing the head of the humerus to be push out the glenoid posteriorly.
POSTERIOR DISLOCATION The coracoid process may be prominent. The elbow will be at the side and the hand on the stomach. Attempting to turn the arm out causes shoulder pain.
For any dislocated shoulder, do not try to reduce the joint. Do not pull on the arm. Try to immobilize as best you can (difficult). Medical referral!
Recurrent dislocations have nothing to do with the treatment after the first dislocation. Recurrent dislocations are dependent upon the damage that happens during the first dislocation.