Download
1 / 27
270 likes | 393 Vues
A 20-year-old woman presented with a growing nodule on her nasal skin, initially diagnosed as melanoma. Immunohistological studies were later repeated, leading to the revised diagnosis of Cellular Neurothekeoma (CN). This case highlights the complexities in differentiating CN from melanoma due to overlapping immunohistochemical markers. Factors affecting diagnostic accuracy, including tissue fixation methods and antigen retrieval techniques, are discussed. The case underscores the importance of careful interpretation of immunohistological results to avoid misdiagnoses in dermatopathology.

E N D
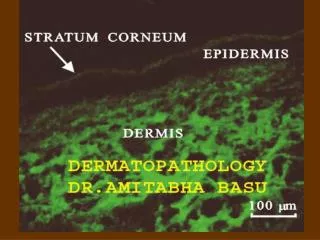
Immunohistology in Dermatopathology: Problem Areas Mark R. Wick, MD www.markwickmd.com
Example Case: A 20 year old woman presented with a 0.6 cm flesh-colored nodule in the left nasal skin, which had slowly enlarged over the previous six months. Physical examination showed no other abnormalities, and the patient was otherwise well. The lesion was removed by excisional biopsy.
After a diagnosis of melanoma had been made, the patient was referred to the presenter’s institution for sentinel lymph node biopsy and possible enrollment in a vaccine trial. However, in light of the patient’s young age and the unusual clinical appearance of the lesion, the attending dermatologist (who is also trained in dermatopathology) asked whether the immunohistological studies might be repeated.
Repeated S100 Stain S100A6 Stain
Cellular Neurothekeoma (CN): Characteristics • Proposals have been made suggesting that CN is a neural-neuroendocrine, or melanocytic, or “fibrohistiocytic,” or hybrid lesion with respect to its lineage of differentiation. • Phenotypically, CN may be reactive for muscle-specific actin; NKI/C3 (a melanocyte-related marker); microophthalmia-transcription factor (another melanocyte-related moiety); protein gene product 9.5 (a neural/neuroendocrine marker); neuron-specific enolase; p63; CD10; podoplanin; and S100A6, a specific calcium-binding S100 isoform. However, it consistently lacks generic S100 protein-positivity, as well as HMB45, melan-A, KBA-62 antigen, PNL2 protein, and tyrosinase, as seen in true melanomas.
Cellular Neurothekeoma:IHC Comparisons with Melanoma • A particular problem is the sharing by both CNs & melanomas of several markers other than S100 protein, such as MITF, NKI/C3, & NSE, ; melanomas also consistently manifest S100A6, and may demonstrate unexpected immunoreactivities (e.g., for myogenous, neural, or epithelial determinants) because of the presence of divergent differentiation.
Was There a Problem in Immunohistochemical Technique or Interpretation in This Case? If So, What Was It?
Preanalytical Factors in Immunohistology • Presumptions holding that advancements in laboratory technique can compensate for all variations in tissue fixation are tantamount to “magical thinking.” • Tissues which are not placed in fixative for a prolonged period after excision will demonstrate a notable deterioration in antigenicity. • Moreover, the particular typeof fixative—e.g., coagulating (Bouin’s solution; ethanol; Carnoy’s solution; B5 solution; Zenker’s fixative), non-coagulating/cross-linking (formalin; glutaraldehyde; paraformaldehyde), or neither (microwave fixation)—has a potentially-major influence on the preservation of various protein molecules. • One can usually control the variable of fixation reasonably well inside a regional healthcare system, but when case material is received from laboratories in other locales it is often impossible to know how that tissue has been preserved and processed.
Formalin B5 Poor fixation Microwave
Analytical Factors in Immunohistology • One sees differing efficiencies of clearing agents (e.g., Histoclear, Americlear, xylene, toluene, etc.)in wax removal from paraffin sections, and variable potential effects on the integrity of tissue proteins. • Antigen “retrieval” steps– microwave-mediated; using vegetable steamers or pressure cookers; employing differing buffer solutions. • Antigen retrieval methods have variable effects on different protein groups, sometimes enhancing immunoreactivity; sometimes decreasing it; sometimes not altering it appreciably. • Several different antibody reagents to any given marker are now available in most instances.
Pankeratin- No antigen retrieval Pankeratin- With antigen retrieval
Iterations in IHC Procedure • Peroxidase-antiperoxidase (PAP) • Avidin-biotin-peroxidase complex (ABC) • Alkaline phosphatase-antialkaline phosphatase (APAAP) • Glucose oxidase-antiglucose oxidase (GAG) • Polymer/Micropolymer-peroxidase (PMP) • Combinations (e.g., Avidin-biotin-peroxidase-antiperoxidase [ABPAP])
Chromogenic Intensifiers– Osmium Tetroxide, Nickel Chloride, Copper Sulfate, Etc. Used to darken and accentuate immunostaining product, but can also increase the level of “background” noise
Why Do We Use So Many Immunostains Currently in Diagnostic Dermatopathology? • There is an increasing “de-morphologicalization” of the training of residents in anatomic pathology & dermatopathology. • This leads to overuse of, & overreliance on, adjunctive laboratory techniques, including immunohistology. • One often fails to see a logical grouping of biological markers in the procurement of immunostains, because of the lack of a sufficiently narrow morphological differential diagnosis. • All of these factors conspire to produce IMMUNOCONFUSION.
?? ?? ?? ??
Two Useful Rules to Bear in Mind in Diagnostic Immunohistology • The Rule of Prior Probability– If one is already certain of a conclusion, the procurement of additional data can only result in confusion, not enlightenment. • Miller’s Rule (for Dr. Rod Miller)-- “True positive” immunostains exhibit cell-to-cell heterogeneity in labeling, whereas “pseudo-positive” reactions are diffusely homogeneous.
Original S100 Repeated S100
Basic Guidelines for the Ordering & Interpretation of Diagnostic Immunostains • Base the selection of stains on a morphologically-sound &suitably-narrow differential diagnosis; • Choose only those studies that will provide a high level of diagnostic discrimination between the pathologic entities being considered—the fewer stains the better; • Neverput great weight on a single immunostaining result if it blatantly contradicts the bulk of the other clinicopathologic data in the case at hand; • Do not use the results of technically-equivocal immunostains to contribute to a diagnostic conclusion.
What Can be Said of Interpretative “Error” in Regard to Entities Such as Cellular Neurothekeoma, Which Have Somewhat Nebulous Diagnostic Criteria? “…If one concludes that anatomic pathology currently lacks precise or accurate criteria relating to certain diagnoses, a situation exists that is comparable to a lack of effective therapy for a particular disease… Yearning for a definitive pathologic diagnosis does not substitute for reality, when no certain method to achieve that interpretation can be found.” (Foucar E: Classification of error in anatomic pathology: a proposal for an evidence-based standard. Semin Diagn Pathol 2005; 22: 139-146.)


![[PDF READ ONLINE] Barnhill's Dermatopathology, Fourth Edition](https://cdn7.slideserve.com/12518495/slide1-dt.jpg)
![[PDF] DOWNLOAD Barnhill's Dermatopathology, Fourth Edition](https://cdn7.slideserve.com/12521186/slide1-dt.jpg)