Download
1 / 31
310 likes | 458 Vues
Alcohol-use disorders: preventing harmful drinking. Workshop on putting NICE guidance into practice . 2 nd . Edition – August 2011. NICE public health guidance 24. What this presentation covers. Background Policy recommendations Pre-training quiz Practice recommendations

E N D
Alcohol-use disorders: preventing harmful drinking Workshop on putting NICE guidance into practice 2nd. Edition – August 2011 NICE public health guidance 24
What this presentation covers • Background • Policy recommendations • Pre-training quiz • Practice recommendations • Post-training quiz • Discussion & other NICE resources
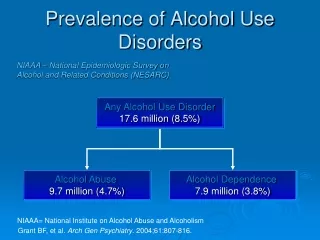
Background • Alcohol is attributable for: • 14,982 deaths in England (2005) • 500,000 recorded crimes (England) • up to 35% of attendances at hospital emergency departments (2003) • 24% of adults drink a hazardous or harmful amount
Recommendations for policy[Please remove this text **this is an alternative slide if running a shorter lunchtime session] • Recommendations 1 to 3 cover: • price • availability • marketing
Policy: price • Consider introducing a minimum price per unit • Regularly review the minimum price per unit • Regularly review alcohol duties
Policy: availability • Consider revising licensing legislation to ensure: • links between the availability of alcohol and alcohol-related harm are taken into account when licence applications are considered • immediate sanctions can be imposed on premises in breach of their licence • health bodies are ‘responsible authorities’
Policy: marketing • Consider a review of the advertising codes – to ensure: • limits set by Advertising Standards Authority for the proportion of the audience under age 18 are appropriate • children and young people are adequately protected where alcohol advertising is permitted • a stringent regulatory system covers all alcohol marketing, particularly via new media
Recommendations for practice • Organisational issues • Children and young people aged 10 to 15 • Young people aged 16 and 17 years • Adults
Organisational issues: licensing • Map alcohol-related problems before developing or reviewing a licensing policy • In ‘saturated’ areas adopt a ‘cumulative impact’ policy • Identify and take action against premises making illegal sales • Ensure sanctions are fully applied
Organisational issues: resources for screening and brief interventions • Prioritise alcohol-use disorder prevention as an ’invest to save’ measure • Conduct a local joint alcohol needs assessment • Include screening and brief interventions in commissioning plans • Provide resources for tier 2, 3 and 4 alcohol services to accommodate a likely increase in referrals
Children and young people aged 10 to 15 years • Routinely assess their ability to consent to treatment • Obtain a detailed history of their alcohol use • Use professional judgement to decide what actionto take • Consider referral to CAMHS, social care or young people’s alcohol services, if there is risk of harm • Tailor discussions to age and ability
Young people aged 16 and 17: screening • Complete a validated alcohol screening questionnaire such as AUDIT • Focus on groups at increased risk of alcohol-related harm • Tailor discussions to age and ability • Routinely assess their ability to consent to treatment
Screening AUDIT – CFor people aged 16 years and over • Scoring:A total of 5+ indicates increasing or higher risk drinking.
Young people aged 16 and 17: extended brief interventions • Ask their permission to arrange an extended brief intervention with a trained member of staff • Provide information on local specialist addiction services to those who do not respond well to discussion but who want further help • Assess the physical and mental health of those who are actively seeking help, or refer them for appropriate treatment and care
Adults: screening Conduct alcohol screening as part of routine NHS practice. If universal screening is not feasible focus on those: • with relevant physical or mental health conditions • who have been assaulted • at risk of self-harm • who regularly experience accidents or minor traumas • who regularly attend GUM clinics or repeatedly seek emergency contraception
Adults: screening • Non-NHS professionals should focus on groups at increased risk of harm from alcohol and people who have alcohol-related problems.For example those: • at risk of self-harm • involved in crime or other anti-social behaviour • who have been assaulted • at risk of domestic abuse • whose children are involved with child safeguarding agencies • with drug problems
Adults: screening • Ensure discussions are sensitive to the person’s culture andfaith and tailored to their needs • Complete a validated alcohol questionnaire • Do not offer simple brief advice to anyone who may be dependent on alcohol • Biochemical measures should not be used as a matter of routine for screening
Adults: brief advice Offer a session of structured brief advice on alcohol Use a recognised resource based on FRAMES principles Where there is an ongoing client relationship, routinely monitor progress
There are times when you will be at risk even after one or two units. For example, with strenuous exercise, operating heavy machinery, driving or if you are on certain medication. If you are pregnant or trying to conceive, it is recommended that you avoid drinking alcohol. But if you do drink, it should be no more than 1-2 units once or twice a week and avoid getting drunk. Your screening score suggests you are drinking at a rate that increases your risk of harm and you might be at risk of problems in the future. What do you think How many units did you drink today? 1 very small glass of wine 1 single measure of spirits Half pint of regular beer, lager or cider 1 small glass of sherry 1 single measure of aperitifs (9%) ...and each of these is more than one unit 3 A pint of “strong”/”premium” beer, lager or cider Alcopop or a 275ml bottle of regular lager A pint of regular beer, lager or cider 440ml can of “regular” lager or cider 440ml can of “super strength” lager 250ml glass of wine (12%) Bottle of wine “regular” (12.5%)
The benefits of cutting down • Psychological/Social/Financial • Improved mood • Improved relationships • Reduced risks of drink driving • Save money • Physical • Sleep better • More energy • Lose weight • No hangovers • Reduced risk of injury • Improved memory • Better physical shape • Reduced risk of high blood pressure • Reduced risk of cancer • Reduced risks of liver disease • Reduced risks of brain damage What’s everyone else like? % of Adult Population What targets should you aim for? Men Should not regularly drink more than 3–4 units of alcohol a day. Women Should not regularly drink more than 2–3 units a day ‘Regularly’ means drinking every day or most days of the week. You should also take a break for 48 hours after a heavy session to let your body recover. Abstain- ers Lower risk Increasing risk Higher risk • Making your plan • When bored or stressed have a workout instead of drinking • Avoid going to the pub after work • Plan activities and tasks at those times you would usually drink • When you do drink, set yourself a limit and stick to it • Have your first drink after starting to eat • Quench your thirst with non-alcohol drinks before and in-between alcoholic drinks • Avoid drinking in rounds or in large groups • Switch to low alcohol beer/lager • Avoid or limit the time spent with “heavy” drinking friends What is your personal target? This brief advice is based on the “How Much Is Too Much?” Simple Structured Advice Intervention Tool, developed by Newcastle University and the Drink Less materials originally developed at the University of Sydney as part of a W.H.O. collaborative study.
Adults: extended brief interventions Adults who have not responded to brief structured advice should be: • offered an extended brief intervention to help address their alcohol use • followed up and assessed
Referral Consider referring for specialist treatment if they: • show signs of moderate or severe alcohol-dependence • have failed to benefit from structured brief advice and an extended brief intervention and still want help • show signs of severe alcohol-related impairment or have a related co-morbid condition
Discussion • Who leads our local joint alcohol needs assessment? • When were our local alcohol care pathways last reviewed? How can we incorporate alcohol screening within routine appointments? • What are the challenges involved in deliveringbrief interventions within routine practice?
NHS Evidence Visit NHS Evidence for the best available evidence on all aspects of harmful alcohol use Click here to go to the NHS Evidence website
Find out more • Visit www.nice.org.uk/guidance/PH24 for the: • guidance • quick reference guide • business case • training plan • audit support • self-assessment tool
What do you think? Has this slide set met your requirements, and will it help you to put the NICE guidance into practice? We value your opinion and are looking for ways to improve our implementation tools. Please complete this short evaluation form. If you are experiencing problems accessing or using this tool, please email implementation@nice.org.uk To open the links in this slide right click over the link and choose ‘open hyperlink’