Download

1 / 1
10 likes | 85 Vues
Explore using theoretical models to improve attendance at cardiac rehabilitation, addressing key barriers and incentives through multifactorial and complex strategies. Design an effective intervention utilizing the Theory of Planned Behavior and Common Sense Model. Refine the intervention by consulting experts, patients, and rehabilitation staff. Translate theories into a tailored letter to motivate patients and provide essential information. Discuss the methodological approach and potential for replication in complex interventions. Considerations include evidence-based development, context relevance, and cost-effectiveness. Evaluation planned through a randomized trial.

E N D
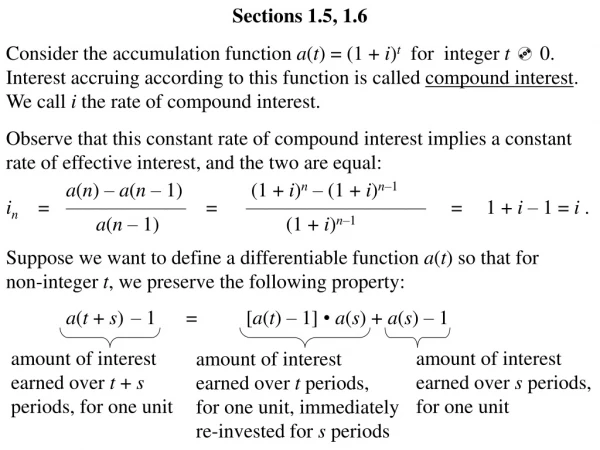
Improving the uptake of cardiac rehabilitation: using theoretical modelling to design an intervention • Mosleh S1, Campbell N2, Kiger A1, • 1Centre for Advanced Studies in Nursing, Department of General Practice & Primary Care, University of Aberdeen, UK. 2 Department of General Practice & Primary care, University of Aberdeen, UK • Introduction • Worldwide, cardiac rehabilitation programmes face the problem of low attendance with typically fewer than 35% of eligible patients attending.1 • In common with other interventions which attempt to influence patient behaviour, increasing attendance at cardiac rehabilitation has proven difficult. • For an intervention to be effective, it will have to provide incentives and tackle key barriers to attendance, thus it will be multifactorial and complex. • Current recommendations are that interventions which attempt to tackle such problems should be developed using theory, evidence, and modelling. 2 • Aim • To design a theoretically based intervention to improve attendance at cardiac rehabilitation. • Methods • 1. Identify theories that might explain patients’ attendance under the following criteria: • Whose constructs map onto factors found to be associated with cardiac rehabilitation. • That have been found to predict attendance at cardiac rehabilitation. • That have been used previously to develop interventions that have improved attendance at cardiac rehabilitation. 2.Conceptualise the intervention • By identifying the factors and pathways that cause and sustain the problem of low attendance at cardiac rehabilitation, and modelling how intervening will modify these factors and pathways. 3. Refine the intervention with three groups: • A panel of five experts from health services research, cardiac rehabilitation and health psychology. • A patient group (25 participants at the hospital programme). • Cardiac rehabilitation staff (nurse, physiotherapist, and psychiatric nurse). • Results • 1. Identifying relevant behavioural theory • Theory of Planned Behaviour (Figure 1) and Common Sense Model of illness representation (Figure 2) were selected as the theoretical bases for the intervention.3,4 • 2. Conceptualizing the intervention • Theory of Planned Behavior (TPB) • Strengthen patients’ beliefs regarding the positive consequences of attending CR and reduce their beliefs about negative consequences. • Strengthen the recommendations from health team members and, if possible, friends and relatives. • Common Sense Model (CSM) • Provide a clear picture about cardiac disease processes, cardiac rehabilitation and treatment strategies. • Figure 1. The Theory of Planned Behaviour Figure 2.Common Sense Model of Illness Representation • Translating theories into an intervention • A theoretically worded letter was selected as the mode of delivery and aimed to • Motivate patients through professional recommendation. • Provide simple information on the contents of the cardiac rehabilitation programme. • Reassure participants that they would receive a tailored programme according to their personal needs in a safe supervised environment. • Inform patients about the benefits of attending the rehabilitation programme. Table 1. Construction of the intervention letter • Discussion • Current recommendations are that interventions which attempt to tackle such problems should be developed using theory, evidence, and modelling. • We report a method for doing this, and believe our methods could be replicated for other complex interventions. • Key activities were literature review, expert meetings, and modelling of how the intervention would work, with due consideration given to the context of the problem and cost of tackling it. • Key tasks were identification of evidence, selection of relevant theory, identification of target points for intervention, and translation of a theoretically modelled intervention into a practical one. These activities and tasks were conducted together and we found them to be synergistic. • The letters and the leaflet will now be evaluated in randomised trial. • In conclusion, a theoretically worded letter and leaflet could be an inexpensive intervention to improve attendance at cardiac rehabilitation. References • Bethell H. The BACR database of cardiac rehabilitation units in the UK. Coronary Health Care 2000; 4: 92-95. • Campbell M, Fitzpatrick R, Haines A et al. Framework for design and evaluation of complex interventions to improve health. British Medical Journal 2000; 321: 694–96. • Ajzen I. The theory of planned behaviour. Organisational Behaviour and Human Decision Processes 1991; 50:179-211. • Leventhal, H., Nerenz, D. The assessment of illness cognition. Measurement Strategies in Health Psychology. In P Karoly (Ed); New York: John Wiley, 1985; 517-554. Centre for Advanced Studies in Nursing