Development of the Heart
290 likes | 836 Vues
Development of the Heart . ANHB 2212 – 2006 – Week 5 Avinash Bharadwaj. Retrospect….

Development of the Heart
E N D
Presentation Transcript
Development of the Heart ANHB 2212 – 2006 – Week 5 Avinash Bharadwaj
Retrospect… The development of the heart is the first of the series of topics that deal with the embryology of organs and systems. This part of embryological study is often called systemic or ‘special’ embryology or organogenesis, as opposed to ‘general’ or early embryology. Throughout systemic embryology, we need to recognise that the starting point is the formation of the trilaminar embryo, that is, a flat embryo with three germ layers – ectoderm, mesoderm and endoderm. At the extreme head end of the embryo the ectoderm and endoderm are in contact without intervening mesoder. This area is called the prochordal (“in front of the notochord”) plate. We have mentioned earlier that the lateral plate mesoderm splits to form the coelomic cavity. Further, the head and tail ends of the embryo undergo folding. The embryo also folds on the sides (lateral folds). Folding of the embryo converts it from a flat plate into a tube.
Cardiovascular System Cardiovascular system includes the heart and the blood vessels. A detailed description of regional blood vessels is beyond the scope of this unit, and we restrict ourselves to the development of the heart. Embryonic development of any organ involves complex processes. Given this complexity, it is amazing that a vast majority of human beings are born without any of the steps going wrong. However, these errors of development do occur; at the gross, histological and even molecular level. An in-depth study of these errors is the subject of advanced study, largely in the medical context. In this unit, we shall mention some of the inborn defects (“congenital defects”) to illustrate some principles. This applies to the development of the heart. On the other hand, from a scientific perspective, the development of the heart does have an interesting evolutionary story to tell. From the Level 1 units and the gross anatomical study last week, we need to recapitulate some basic anatomical facts about the heart. We know that the heart has two receiving chambers (atria) and two pumping chambers (ventricles), with partitions or septa (singular – septum) between right and left chambers. We also understand the precise distinction between arteries and veins as vessels bringing blood towards the heart and taking it away from the heart respectively.
Foetal Body RA RV Lungs LA LV Body Postnatal vs Foetal Circulation • Postnatal Body RA RV Lungs LA LV Body The basic difference between postnatal and foetal circulation is that foetal lungs are nonfunctional. Effectively, blood from the right side of the heart has nowhere to go and needs to be ‘shunted’ to the left. Such a shunting passage exists between the right and the left atria. However, if no blood flows through the right ventricle, that chamber will fail to develop. Thus some blood does pass to the RV. As it is pumped into the pulmonary artery, it needs to be shunted again, this time to the aorta. This illustrated below. But we are jumping too far ahead! This was mentioned as one of the basic principles of the development of the heart…let us begin at the beginning.
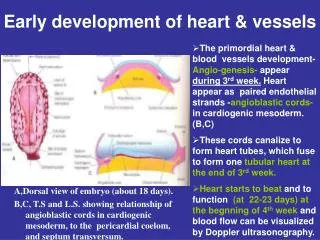
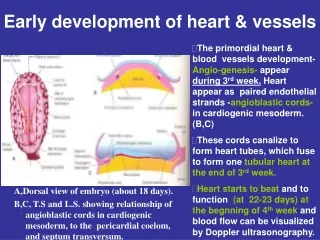
H Prochordal plate Cardiogenic area Earliest Development Cardiovascular system makes its first appearance while the embryo is still flat. Clusters of mesodermal cells specialise to form blood cells. Mesodermal cells around these flatten to form endothelium of blood vessels. These clusters are called blood islands of angiogenic (“blood vessel-forming”) cell clusters. In the accompanying diagram note that these form a curve reaching well beyond the neural plate and the notochord. A mass of mesoderm, called cardiogenic area, near the head end (H) will give rise to the heart. The sagittal section below illustrates the three germ layers, prochordal plate and the cardiogenic area.
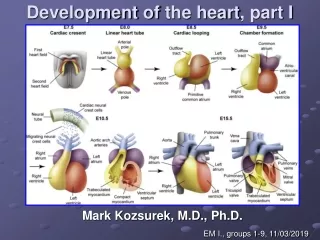
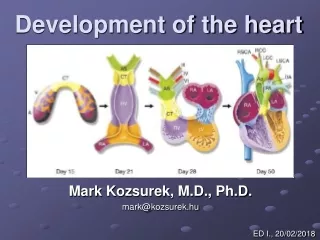
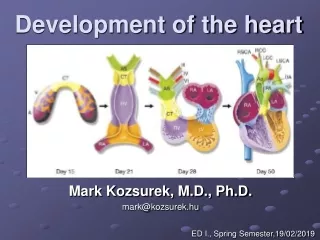
Heart Tube Head Fold With the formation of the head fold (shown in the blue circle), note how the cardiogenic area changes its position. Also observe that the endoderm (yellow) is beginning to form the gut tube. At this stage only the head and tail ends of the digestive tube are recognisable. In the lowest picture, the gut tube is better seen and the heart is in fact in the form of a tube (red).
Heart Liver The Heart Tube In the picture on the left the relationships of the heart, the gut tube and the liver are clearer. In the magnified picture of the heart tube, the tail end is the venous end and the cranial end is the arterial end. The changing shape of the tube also makes it possible to recognise the primitive chambers of the tube. Remember that the tube is not partitioned at this stage. Hereafter, for descriptive convenience, we shall view this tube in the vertical position, with the caudal (venous) end below and the cranial (arterial) end at the top as shown below.
B V D A V SV The Tube Bends This picture shows three successive stages in the growth of the tube. The tube, as it grows, cannot be accommodated within the pericardial cavity and undergoes bending. The primitive chambers of the heart are recognisable, and are labelled in the last picture. SV – sinus venosus (receives veins from the body), A – atrium, V – ventricle. The ventricle continues into the ‘bulbus cordis’which in turn leads to the arterial end. Two terms are used somewhat confusingly for the parts at the arterial end. These are conus arteriosus and truncus arteriosus. In our discussion we shall simply say ‘arterial end’ of the heart.
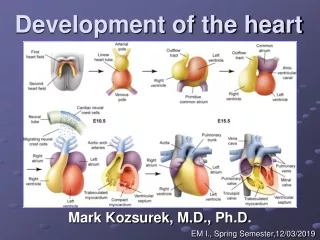
A A A B-V Loop V Left view Front view The Chambers Recognise the chambers in these two views. In the view from the left side, the sinus venosus is partly hidden. Note that with the bending of the tube the atrium is now dorsal and the loop formed by the ventricle and the bulbus cordis (bulbo-ventricular loop) is ventral. In the next slide we shall examine the interior of the unpartitioned heart.
A-Ar LA RA AVC The Interior A portion of the ventral wall of the bulbo-ventricular loop is removed to show the interior. Since there is no partition, there is a single passage from the atrium to the ventricle. This passage is the atrioventricular canal. Note the direction of blood flow through the bulboventricular loop. Also note that the single vessel leading out of the heart has given rise to what are called aortic arches.
Left – Right Partitioning • Interatrial septum • Interventricular septum • Spiral (aortico-pulomonary) septum • Endocardial cushions (A-V cushions) • Functional requirements • There must always be a right to left passage!
Interatrial septum • Partitioning • Right to left passage • Mechanism for closing the passage
A V
Septum Primum • This is a sagittal section seen from the right. AVC V
Foramen Primum • Foramen primum : Between the septum and the AV Cushions
Passage is a Must! • Foramen secundum • Foramen primum about to disappear
Septum Secundum • To the right of primum • Foramen primum has disappeared
Foramen ovale • F. Ovale – • In septum secundum • Further…
The ‘Valve’ • Two septa • Two foramina
Sinus Venosus • Originally a symmetrical structure • Venous return more to the right • Left horn becomes smaller • Opening shifts to the right • Later – part of right atrium
Left Atrium • Four pulmonary veins • Common opening • “Absorption” of veins into atrium • Rough part - auricle
The Ventricular Septum Three Parts • Interventricular septum • AV Cushions • Spiral Septum
R Membranous Spiral (Aorticopulmonary) Muscular Ventricular Septum
Foetal Circulation • Very little pulmonary flow • Placental Circulation • Right to Left Passages
IVC : Blood from placenta • Ductus venosus • F. ovale • Ductus arteriosus
Changes At Birth • Closure of interatrial septum • Closure of ductus arteriosus • Closure of ductus venosus
Congenital Heart Disease • Septal Defects – Atrial and Ventricular • Endocardial cushion defects • Aorticopulmonary defects • PDA • Others Last Slide