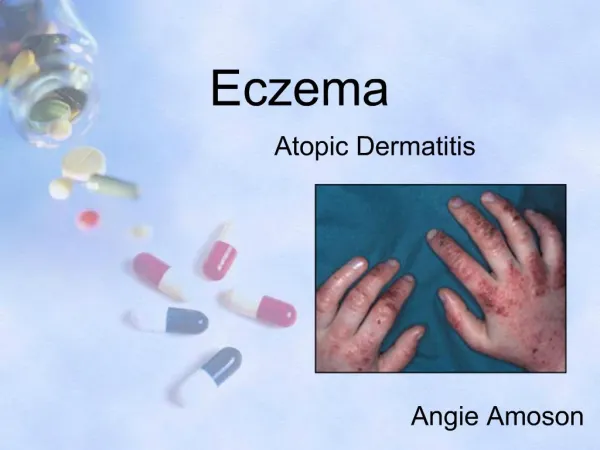
ECZEMA
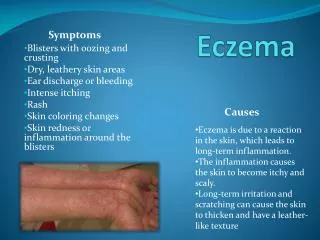
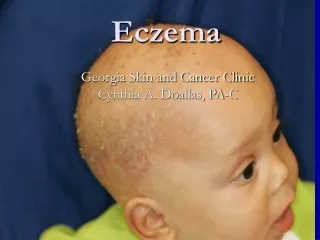
ECZEMA. Introduction Case Scenarios Conclusions. Introduction. Eczema = Dermatitis. Effect on Quality of Life (Burden of Disability). 10-15% children suffer from atopic dermatitis Asteototic dermatitis is becoming more and more common in the elderly

ECZEMA
E N D
Presentation Transcript
Introduction • Case Scenarios • Conclusions
Effect on Quality of Life(Burden of Disability) • 10-15% children suffer from atopic dermatitis • Asteototic dermatitis is becoming more and more common in the elderly • Hand dermatitis is a major cause of absence from work
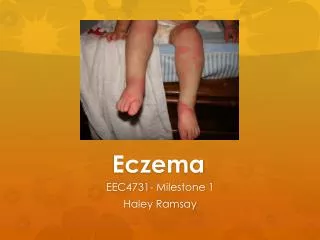
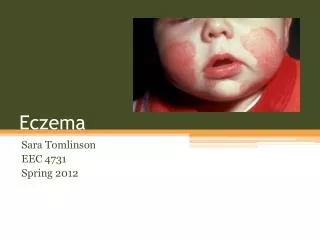
Case 1 • 6 months old child • Onset of problems at age 2 months • Formula fed child-several changes in milk tried • “None of the ointments work”
Sleeping poorly • Allergy tests?
Basic Management of Atopic Dermatitis • Explanation – expectations of treatment • Emollients • Topical Corticosteroids
Explanation • Incredibly common • Cause unknown – NOT allergy • Self-limiting in most cases (eventually) • Waxing and waning natural history
Emollients • Bath • General • No limit to their use
Topical Corticosteroids • Mainstay of treatment • Not dangerous if properly used • Most “steroid phobias” allayed by explanation • Awareness of different strengths
Package of Care • Time • Explain • Prescribe a package of emollient(s) and topical steroid(s) • Empower the parents to alter strengths of corticosteroids depending on clinical severity
Role of Nursing Colleagues • Ideal disease for follow-up by practice nurses and health visitors • Offer support through chronic disease • Easy access for flares of disease • Support from specialist dermatology nurses in secondary care
What about Infection? • Staphylococcus aureus on 100% of skin lesions • But antibiotics don’t cure atopic dermatitis • But some cases improve when either topical or systemic antibiotics added
Eczema Herpeticum • Unwell patient • Severe pain • Typical umbilicated, coalescing papules • Herpes simplex virus (usually type 1) • Urgent hospital admission
What to Try if Adequate control NOT Achieved • Concordance (social issues) • Infection • “Pulse” of stronger topical corticosteroid • Bandaging • Referral
Case 2 • 75 year old man • Retirement apartment • Likes to keep clean • Diuretics • Itching started on legs and spread to arms and trunk
Pathogenesis • Dryness and suppleness = state of hydration of Stratum corneum • State of hydration of stratum corneum dependant on rate of migration of water through stratum corneum and rate of evaporation from its surface • Natural level of skin lipids decreases as age increases
Management • Is the patient clinically or sub-clinically dehydrated? • Is the environment too dry? • Is the skin being degreased too frequently or too harshly?
Emollient • Topical corticosteroid – dip in and out after initial pulse
Case 3 • 40 year old man • “Fed-up” with years of dandruff • Recent onset of itchy, red scaling of eyebrows, naso-labial folds
Pathogenesis • Tentative • Increased numbers of Pityrosporum ovale coupled with ? Genetic tendency
Treatment • Targeted against both P.ovale and inflammation • Chronic condition therefore need for repeated periods of treatment
Anti-Pityrosporum shampoo eg Selsun, Head & Shoulders, Nizoral (contact time) • Combination anti-Pityrosporum and anti-inflammatory cream eg Cannesten HC, Daktacort, Nizoral
Case 4 • 35 year old car mechanic • “Eczema” as a toddler but clear for years • Recent onset dry, itchy, red rash both hands • Some improvement when goes on holiday
Hand dermatitis • Multifactorial • Endogenous • Irritant • Allergic • Infection – Bacterial and Fungal
Management • Package of treatment • Address any precipitating cause • Scrapings for mycology and swab for bacterial contamination/infection if indicated • General hand care • Emollients • Topical Corticosteroid
Conclusions • Diagnosis • Precipitating causes • Time for explanation – natural history • Empower the patient to treat their disease • Package of treatment • Point of follow-up
What to Try if Adequate control NOT Achieved • Concordance (social issues) • Infection • “Pulse” of stronger topical corticosteroid • Bandaging • Referral