Thyroid and Parathyroid Glands
420 likes | 765 Vues
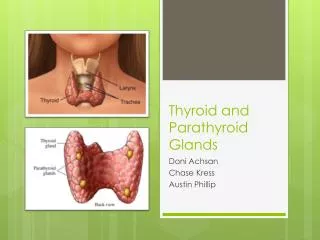
Thyroid and Parathyroid Glands. NUR 111. Functions of the Thyroid. Pg. 1450 Metabolic rate Regulate protein, carbs and fat metabolism Increase RBC production Inc bone formation, decrease bone resorption of Ca +. Regulation of Metabolism. Hormones T 3 & T4 increase BMR

Thyroid and Parathyroid Glands
E N D
Presentation Transcript
Thyroid and Parathyroid Glands NUR 111
Functions of the Thyroid • Pg. 1450 • Metabolic rate • Regulate protein, carbs and fat metabolism • Increase RBC production • Inc bone formation, decrease bone resorption of Ca+
Regulation of Metabolism • Hormones T3 & T4 increase BMR • Secretion controlled by hypothalamic-pituitary-thyroid gland axis • TRH » TSH » T3 & T4 (neg feedback) • Protein and Iodine very important for T3 & T4 production
Calcium and Phosphorus Balance • Calcitonin (thyrocalcitonin, or TCT) • Reduces bone resorption, lowers serum Ca+ • Low serum Ca+ suppress TCT: • Elevated serum Ca+ trigger TCT
Causes of Hyperthyroidism • Pg. 1482 • Graves’ disease (Autoimmune) • Toxic multinodular goiter • Thyroid adenoma (benign tumor) • Pituitary hyperthyroidism • Excessive use of thyroid hormone
Hyperthyroidism • More common in women • Lab assessment p.1485: T3, T4 • TSH (Graves’) • Thyroid Scan (RAIU) = increased
Nursing Diagnosis • Depends on condition of client • Possible Dx. Include • Imbalanced nutrition: > body requirements • Fatigue • Anxiety • If large goiter present: what is priority???
Interventions • Nonsurgical: monitor V/S, rest, cool environment • Medications: PTU (propylthiouracil), SSKI, beta blockers • Radioactive Iodine Therapy • Remember eye care
Interventions • Surgical: total or subtotal thyroidectomy • Preop = antithyroid meds, SSKI • Postop = very important • Monitor for Bleeding, respiratory distress, tetany, weak voice, thyroid storm (p.1487)
Causes of Hypothyroidism • Pg. 1489 • Removal or destruction of thyroid • Autoimmune (Hashimoto’s Disease) • Iodine deficiency • Medications (ex.Lithium)
Hypothyroidism • More common in women • Lab assessment: T3, T4 • TSH • Monitor for depression
Nursing Diagnosis • Decreased cardiac output • Ineffective breathing pattern • Altered thought process • Constipation
Interventions • Levothyroxine sodium (Synthroid) • Avoid sedatives & narcotics • Monitor vital signs • Monitor for S&S of hyperthyroidism • Family teaching re: mental status
Myxedema Coma • Hypothyroid Crisis --> rare but serious • Etiology: • acute illness/ trauma • * rapid withdrawal of thyroid meds. • use of sedatives / narcotics • surgery • exposure to cold
Myxedema Coma • temp / BP • Na+ • blood glucose • Lactic acidosis • Coma
Collaborative Nursing Care • IVF • Airway • IV: • Synthroid • Glucose Warming blanket
Acute Bacterial Pain Temp. Malaise Dysphagia TX Antibiotics Subacute Viral Temp. Chills Pain in jaw and/or ear TX ASA and steroids Thyroiditis
Thyroid Cancer • Painless nodule in thyroid • Treatment : • RAI • Surgery
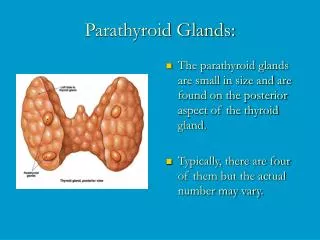
Parathyroid Glands: • 4 in number • can be removed w/ thyroid during surgery • Parathyroid secretes: • Parathyroid hormone (PTH)
REMEMBER : Thyroid -> Calcitonin -> decreases serum calcium PTH - increases serum calcium
Parathyroid Glands: • Major Role: • Regulate blood levels of calcium and phosphate • PTH acts on: • GI tract • Kidney • Bones • If serum CA PTH secretion • PTH - activates Vit. D --Increase calcium absorption from g.i. tract
Remember:Thyroid also secretes Calcitonin • Calcitonin helps--> • keep Ca in bones • maintain balance of Ca and Phosphorus Calcium -- 8.8 - 10.5 • Phosphorus - 3 - 4.5
HyperparathyroidismPathophysiology • PTH secretion = Ca+Phos • increased reabsorption of calcium by kidneys = • increased excretion of Phosphate • Causes • tumors • hyperplasia of parathyroid gland
Data Collection : • PTH • renal calculi • nephrocalcinosis • bone decalcification • serum Ca • GI: anorexia, N&V, epigastric pain, constipation, • M/S: fatigue & lethargy • [serum Ca] > 12 mg/dl = mental status
Complications: • Renal Failure • Fractures • Collapse of vertebra
Collaborative Management :focuses to decrease serum calcium • Diuretic & Fluid Therapy • Lasix /0.9% Na Cl • Drug therapy • Phosphates • Calcitonin -miacalin spray Skel. Release Renal clearance • Calcium Chelators - binds with Ca. -< dec. Levels of free calcium • Parathyroidectomy
Nursing Interventions : • Diuretic & Fluid Rx: • Monitor: • cardiac function • I & O • renal status • serum Ca • Calcium Chelator Rx: • Monitor: • LFT, BUN & Creatinine, CBC
Post - op careParathyroidectomy • Same as thyroidectomy • Monitor for *** Tetany • continuous spasm of hands / feet ---> convulsions • calcium levels • Calcium supplements ( Tums, Oscal ) • Maintain airway
PathophysiologyHypoparathyroidism • PTH • Etiology (rare) • thyroid / parathyroid surgery • Hypomagnesemia • Idiopathic
Data CollectionHypoparathyroidism • Tetany • Check : • Chvostek’s • Trousseau’s • tingling • severe muscle cramping • irritability
Collaborative management of care • IV calcium gluconate • Oscal • Vitamin D • High Calcium diet • Magnesium IM or IV