Material
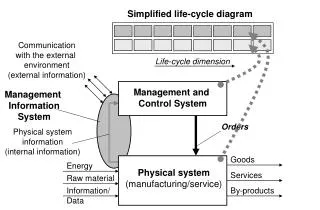
LARGE VESSEL VASCULITIS (GIANT CELL ARTERITIS, TAKAYASU’S ARTERITIS) – EXTENDED CASE REPORT. SŁAWOMIR TYMIŃSKI, ANDRZEJ ŁABYK, ANNA KAPŁAŃSKA. Students Research Group; D epartment of Internal Medicine, Hypertension and Vascular Diseases, Warsaw Medical University, Warsaw, Poland.


Material
E N D
Presentation Transcript
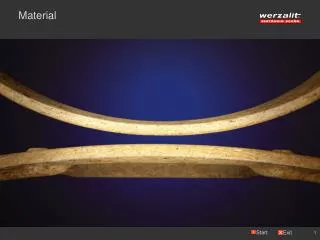
LARGE VESSEL VASCULITIS (GIANT CELL ARTERITIS, TAKAYASU’S ARTERITIS) – EXTENDED CASE REPORT SŁAWOMIR TYMIŃSKI, ANDRZEJ ŁABYK, ANNA KAPŁAŃSKA Students Research Group; Department of Internal Medicine, Hypertension and Vascular Diseases, Warsaw Medical University, Warsaw, Poland Objective Takayasu's arteritis and giant cell arteritis(GCA)are separate, but similar, idiopathic diseases characterized by constitutional symptoms, markers of systemic inflammation and microscopic features of pan-arteritis of large vessels. * Aim To present an analysis of medical records of patients hospitalized due to large vessel vasculitis. * Aortic dissection Material We analysed the medical records of patients hospitalized due to vasculitis and hypertension at the Department of Hypertension between 1998 and 2005 Figure-a 32-year old femaleAortic dissection patient (Takayasu’s a. ) developed aortic dissection revealed in MR • 4pts(3 women, 1 man) met the diagnostic criteria of Takayasu's arteritis and 3 (2 women, 1 man)ofGCA. Thus we performed an analysis of 7 cases (median age 51). • The pts had non-vascular symptoms (arthralgia – 3 pts, myalgia -2 pts, weight loss - 2 pts), vascular stenosis (asymmetric pulses -4 pts, multiple vascular murmur -4pts, absent pulses -2pts) and hypertension due to renal artery stenosis (1 pt). • Disturbed consciousness was observed in 5 pts, visual disturbances in 5 pts, endovascular interventions in 2 pts. Laboratory findings included anaemia (3 pts) elevated CRP (6 pts) and ESR (7 pts). • Almost all patients had multiple sites of arterial involvement and aneurysm formation documented by CT and MRI. Response to corticosteroid treatment was variable, with symptom attenuation (3 pts) and return of pulses (3 pts). • Methods • Physical examination • Visualisation results– arteriographic, Doppler US, CT and MR • ·Laboratory tests- elevated CRP, sedimentation rate and increased immunoglobulin concentration Results • Conclusion • Large vessel vasculitis is a serious systematic disease with considerablecomplications. • 2. Large vessel vasculitis may resemble • other systemic diseases. • 3. Treatment results are non-homogenous.