PULMONARY FUNCTION TESTS
PULMONARY FUNCTION TESTS. DR.MUKHTAR A. ADEIZA DEPARTMENT OF MEDICINE A.B.U.T.H ZARIA THORACIC CLUB MEETING, 19 TH MAY 2011. Introduction. Pulmonary function tests (PFTs) is also referred to as lung function tests. They are useful in defining: Defining respiratory disorders


PULMONARY FUNCTION TESTS
E N D
Presentation Transcript
PULMONARY FUNCTION TESTS DR.MUKHTAR A. ADEIZA DEPARTMENT OF MEDICINE A.B.U.T.H ZARIA THORACIC CLUB MEETING, 19TH MAY 2011
Introduction • Pulmonary function tests (PFTs) is also referred to as lung function tests. • They are useful in defining: • Defining respiratory disorders • Quantifying the severity of deficit • Monitoring the course of disease
Introduction • Simple tests such as spirometry or measurement of peak expiratory flow (PEF) may be performed in consulting room, bed side or by the patient at home • Complex tests require the facilities of a lung function laboratory
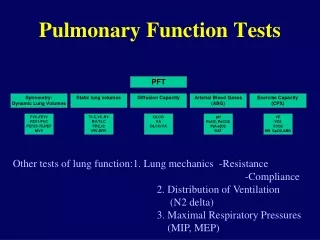
Introduction • Ventilatory Function: Evaluation of this includes assessing volume of gas and rate of movement of gas into and out of the lung: • Common tests are: - Spirometry - Measurement of lung volumes - Quantification of diffusion capacity
Introduction • Normal values depend on the patient`s predicted normal value Clinical Pearl • PFTs should not be interpreted in isolation but should be considered in the context of additional information concerning the patient
Spirometry • Spirometry- Making pulmonary measurements with a spirometer • Spirometer- Any device used for measuring flows and volumes inspired and expired by the lungs • Spirogram- Graphical recording of the forced exhaled volume versus time
Spirometry • Values measured to assess airflow using spirometry are: • FVC - (Forced vital capacity) most important test as it is sensitive to diseases that alter the lungs mechanical properties • FEF25 -75% Maximal mid-expiratory flow rate) • FEV1- (Forced expiratory volume in 1 second) most reproducible and useful test • PEF- Peak expiratory flow rate
Spirometry • Values obtained are interpreted taking into consideration: - age - sex - height - race • Normal if they fall within 80-120% predicted • Below 5 percentile is considered abnormal
Spirometry • Is a measure of airflow and lung volumes during forced expiratory manoeuver from full inspiration. • The measurements are sometimes referred to as dynamic lung volumes • ATS/ERS criteria for acceptable and repeatable spirometry • To obtain an accurate recording the subject should: • Sit up straight • Get a good seal around the mouthpiece of the spirometer • Rapidly inhale maximally • Without delay, blow out as hard and as fast as possible • Continue to exhale until the patient can blow no more • Expiration should continue for at least 6 seconds and up to 15 seconds if necessary.
Manoevres are repeated until at least 3 technical acceptable manoevres (no coughs,air leaks, false starts) are completed • However no more than 8 attempts in total • Spirometry provides 3 basic measurements: • The FVC, the FEV1, the ratio of the FEV1 /FVC or FEV1% • All the 3 measurements are needed to interprete spirometry • A normal spirogram plots the total volume exhaled against time • The trace becomes flat after about 3-4 seconds because the total volume of air which can be exhaled (FVC) is expelled within this time • Approx. 80% of this vol. (slightly lower in older people) is exhaled within 1 second, 0.7- 0.8 or 70-80% • Spirometry can demonstrate 2 basic patterns of disorder – obstructive and restrictive
Spirometry • Most spirometers display the following graphs: • A volume-time curve, showing volume (liters) along the Y-axis and time (seconds) along the X-axis • A flow-volume loop, which graphically depicts the rate of airflow on the Y-axis and the total volume inspired or expired on the X-axis
Measurement of Lung Volumes • Values measured to assess lung volume: - Total Lung Capacity - Functional Residual Volume - Vital Capacity • Measurements of static lung volumes can be helpful in sorting out restrictive and obstructive disorders
Lung Volumes • These are measured under static conditions using: - Helium dilution - Body plethysmography - Nitrogen washout method - Radiographic method
Most important measurements are: • Total lung capacity (TLC): Volume of air in the thorax at full inspiration. This is limited by the mechanics of the chest wall, the respiratory muscles used in inspiration and lung compliance. • Residual volume (RV): Volume of air left in the thorax at full expiration. This is determined by chest wall mechanics, the respiratory muscles of expiration, the elastic recoil of the lungs and in some cases (particularly the elderly and those with airways disease) by airways collapse, usually at the lung bases, preventing further air from escaping. • Functional residual capacity (FRC): Volume of air in the lungs at the end of a normal expiration. At this volume the outward ‘springiness’ of the chest wall balances the elastic recoil of the lungs.
Obstructive pattern of lung diseases • Diagnosed from reduced FEV1/FVC ratio • Usually < 0.7 but may vary with age • FEF25-75% more sensitive for measurement of early airflow obstruction especially small airway, less specific
Obstructive pattern of lung diseases • TLC is normal or increased • RV is increased and the ratio RV/TLC is increased • VC is frequently decreased
Restrictive pattern of lung diseases • Normal or increased FEV1/FVC ratio • Reduction in the TLC • Two types: Pulmonary parenchymal Extraparenchymal • This is based on RV and RV/TLC ratio
Restrictive pattern of lung diseases • Parenchymal: TLC is reduced and the FEV1/FVC is normal or above normal • RV is decreased with low RV/TLC ratio • Extraparenchymal: TLC is decreased but the RV is normal if due to muscle weakness or pleural disease • If due to deformed chest, RV may be increased • High RV/TLC ratio
FEF25-75% • The forced expiratory flow between 25% and 75% of the FVC • This is the slope between the FEF25 and FEF75 • Represents the airflow in the medium and small airways • Sensitive but less reliable indicator of airflow obstruction than FEV1 • May indicate mild airways disease
Reversibility • Reversibility of airflow obstruction is often demonstrated by repeating spirometry after treatment • A dose of inhaled beta-agonist such as salbutamol 2.5mg by nebuliser is administered after an initial test and spirometry is repeated 15-30 mins later. • Ipratropium bromide may be used or spirometry can be repeated after a few weeks of inhaled or oral corticosteroids treatment • Significant reversibility refers to an improvement of 12% or more and 200ml or more in FEV1 • Reversibility is characteristic feature of asthma • Airflow obstruction in COPD is largely irreversible
Clinical conditions Obstructive lung Diseases: • Asthma • COPD • Bronchiolitis • Bronchiectasis • Cystic fibrosis
Clinical conditions Restrictive - Parenchymal: • Sarcoidosis • Interstitial Pulmonary Fibrosis • CT diseases • Pneumoconiosis • Drug/radiation induced lung disease • Asbestosis • Lung resection
Clinical conditions Restrictive Extraparenchymal (Neuromuscular): • Diaphragmatic paralysis • Myasthenia gravis • GBS • ALS • Muscular dystrophies • Cervical spine injury Restrictive Extraparenchymal (Chest wall): • Kyphoscoliosis • Obesity • Ankylosing spondylosis • Ascitis • Pregnancy • Thoracoplasty
Flow-volume loops • Plots airflow on the vertical axis against the total volume exhaled on the horizontal axis. • Useful because different lung disorders produce distinct, easily recognized patterns • Inspiratory manoeuvres can also be plotted on flow-volume loops and this can be occasionally helpful • On the loop, no direct indicator of time and FEV1 cannot be easily measured
Variable extrathoracic obstruction Variable intrathoracic obstruction
Peak Expiratory Flow (PEF) • Most widely used PFT • Used to objectively measure airway obstruction • Simple to perform, cheap, available • Can be performed at home or in the clinics. • PEF is generated in the 1st fraction of a second of a forced expiratory manoeuvre • The disadvantage is that the measurement is very dependent on effort and technique, poor standardization
PEF • The major contribution to the peak flow is from the large central airways • Blow hard into meter after a full inspiration • Record the best of three values • Establish personal best for the patient and use that to assess degree of control/deterioration
PEF • Main value is in the management of asthma • Despite the above limitations, PEF may be used in the: • Diagnosis of asthma. • Assessment of acute asthma • Monitoring of chronic asthma
Diffusion capacity of the lungs for CO (DLco) • The pt breathes air containing a known conc of CO from a douglas bag and expired air is collected in another Douglas bag over a timed period, • The rate of CO transfer can be calculated from the difference btw inspired and expired concs. Reduced DLCO: • Pulmonary thromboembolic disease • Idiopathic pulmonary arterial hypertension • Arteriovenous malformations • vasculitis (for example scleroderma, SLE) • Pneumonic consolidation or areas of lung collapse • Emphysema • ARDS
Fibrotic lung dxes e.g. fibrosing alveolitis, asbestosis • Granulomatous dxes e.g. hypersensitivity pneumonitis, sarcoidosis • Lung resection • Pulmonary oedema • Anaemia • Recent smoking (high CO tension in blood reduces uptake Increased DLCO, conditions that increase the amt of Hb available to bind CO • Polycythaemia • Pulmonary haemorrhage syndromes such as Goodpasture`s syndrome • May also be seen in obesity and asthma
Preoperative PFTs • The goals of preoperative PFTs are: • To detect unrecognized lung disease • To estimate the risk of operation compared to potential benefit • To plan peri-operative care • To estimate postoperative lung function
Preoperative PFTs • Several studies have shown a high prevalence of unsuspected impairment of lung function in surgical patients and suggest that preoperative PFTs is underutilized • There is evidence that appropriate preoperative management improves surgical outcome in patients with impaired lung function
Indications for Preop PFTs • Subject • Known pulmonary dysfunction • Current smoking, if > 1 pack/day • Chronic productive cough • Recent respiratory infection • Advanced age • Obesity > 30% over ideal weight • Thoracic cage deformity such as kyphoscoliosis • Neuromuscular diseases such as ALS or myasthenia gravis
Indications for Preop PFTs • Procedure • Thoracic or upper abdominal surgery • Pulmonary resection • Prolonged anaesthesia
Calculation of lung function after resection of lung tissue Postop FEV1 = Preop FEV1 x no of remaining segments 18 • Thus if 5 segments are removed and the preop FEV1 is 2.0L, the predicted postop FEV1 is: 2 x 18 – 5 = 1.4L 18 • This is the estimated level of lung function after full recovery and not immediately after op • A common recommendation is that surgical resection shouldn’t be performed if postop FEV1 is less than 0.8L
Flow 67yr old man, 86kg, 180cm (L/s) 59 pack yrs of smoking SOB on exertion for 5years Wheezing Volume (L) Normal Observed % pred post-dilator FVC(L) 4.97 2.06 43 2.67 FEV1(L) 3.67 0.56 15 0.75 FEV1/FVC(%) 77 27 FEF25-75 31 0.2 6 MVV(L/MIN) 136 29 21 TLC(L) 7.02 8.64 123 RV/TLC(%) 32 69 216 DLco (ml/min/mmhg) 27 21 79
FLOW Male, 68kg, 186cm (L/s) SOB on exertion Cor pulmonale SpO2 85% Volume (L) Normal Observed % predicted FVC(L) 6.01 1.12 19 FEV1(L) 4.89 1.04 21 FEV1/FVC(%) 81 93 FEF25-75(L/s) 4.6 2.2 48 MVV(L/min) 190 81 43 TLC(L) 7.45 2.09 28 RV/TLC(%) 19 44 232 Dlco (ml/min/mmhg) 35 9 26