
Comprehensive Guide to Back Pain: Causes, Diagnosis, and Management
E N D
Presentation Transcript
BackPain Done By: Abdulrahman Alfowzan Sultan Alzahrani NawafAlzahrani
Objectives • Common causes • Diagnosis including history, Red Flags, Examination • Brief comment on Mechanical, Inflammatory, Root nerve compression, Malignancy • Role of primary health care in management • When to refer to specialist • Preventionand Education
Q1. The two most affected nerve roots in Radiculopathy? • L4 and L5. • L5 and S1. • S1 and S2. • L4 and S2.
Q2. Patient came to the clinic complaining of low back pain, in examination the big toe extension is weak, which nerve root you think is involved? • L3 • L4 • L5 • S1
Q3. Which one of the following is do you think is appropriate to referral ? • Fractures • Caudeequina • A+B • Undiagnosed back pain • All of the above
Q4. What is the most likely diagnosis? • Disc herniation • Vertebral fracture • Spondylolisthesis • Ankylosing spondylitis
Q5: Which of the following is considered as a red flag in patients with back pain: • History of DM • Family history of back pain • Focal neurologic deficit • Young age
Introduction • Back pain is one of the most common condition among all ages regardless of the etiology. • In fact, 8 out of 10 adults will experience an acute episode of back pain at some point in their lifetime. • Fortunately, most episodes of back pain resolve with time: approximately 50% of patients will experience back pain relief within two weeks and 90% within three months. • In USA it is the commonest cause of limitation of activity in those under the age of 45. • InSaudi Arabia Seven studies were cross-sectional found a prevalence and pattern ranging from 53.2%to 79.17%.
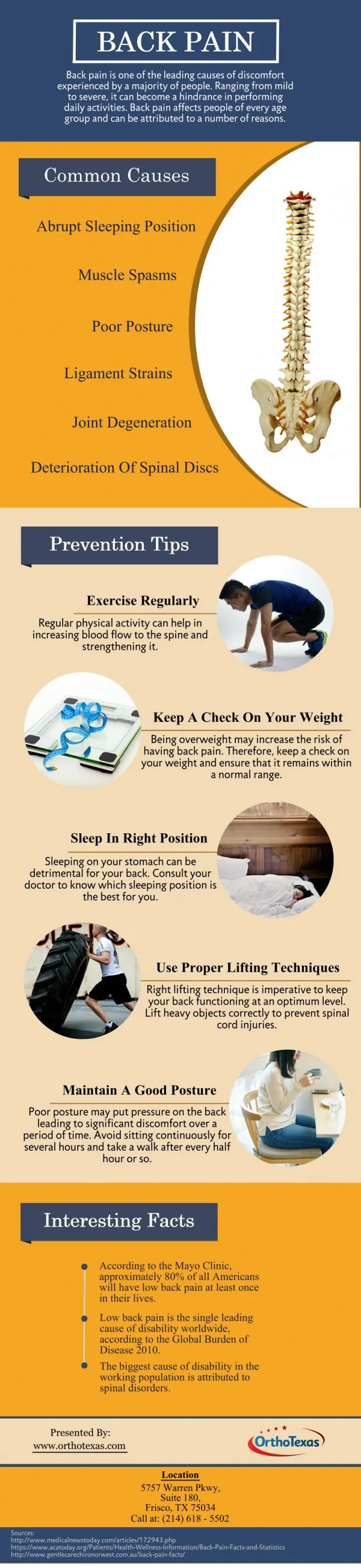
Muscle Strain and Ligament Sprain(Soft tissue injury) A low back sprain or strain can happen suddenly, or can develop slowly over time from repetitive movements. • Strains occur when a muscle is stretched too far and tears, damaging the muscle itself. • Sprains happen when over-stretching and tearing affects ligaments, which connect the bones together. • In fact, back muscle pain is the most common source of back pain but do not sound serious and do not typically cause long-lasting pain
Common causes of sprain and strain include: • Lifting a heavy object, or twisting the spine while lifting • Sudden movements that place too much stress on the low back, such as a fall • Poor posture over time • Sports injuries, especially in sports that involve twisting or large forces of impact Could treat it simply by pain medicines, such as acetaminophen, muscle relaxant and Ice packs.
Degenerative Spinal Disorders (spondylosis) • Degeneration: “deterioration of a tissue or an organ in which its function is diminished or its structure is impaired” Types: • Degenerative disc disease : • Facet osteoarthritis. • Risk factors: 1- Non-Modifiable : • Age-related. • Genetic predisposition • 2- Modifiable: • Smoking. • Obesity. • Previous injury, fracture • Subluxation • Deformity.
1- Mechanical pain: due to joint degeneration or instability. • Activity related-not present at rest. • Associated with movement: • Sitting, bending forward (flexion): apply pressure on the disc “ discogenicpain”. • Standing, bending backward (extension): apply pressure on the facet joints “Facet syndrome” • 2- Neurologic symptoms: due to neurologic impingement: • Can present even at rest.
Spondylolisthesis This condition occurs when one vertebra slips over the adjacent one. Due to: • Defect or fracture of the pars (between the facet joints) • Mechanical instability of the facet joints (degenerative). • Joint damaged by an infection or arthritis • The pain can be caused by instability (back pain) • Compression of the nerves (Radiculopathy) • Aggravatedby: prolonged standing, walking and exercise.
Ankylosing spondylitis • Spine fusion • Many genes can cause it but the major gene that causes this disease is HLA-B27. • Age <40 • Improved with exercise • Pain at night and morning stiffness
Deformities • Scoliosis: Abnormal lateral curvature • of the spine • Kyphosis: Anterior wedging
Tumors • Most tumors in the spine are metastatic. • It is important to detect early as possible because of the effect of a delayed diagnosis on treatment and prognosis. • The neurological signs will be progressive. • history of malignancy, six main primary malignancies that metastasize to the spine from (prostate, breast, lung, thyroid, kidney and melanoma). • Symptoms include:- • Gradually Worsening back pain. • Aggravated by lying down. • Limb paresthesia or weakness. • Fever, weight loss.
Vertebral Fractures Causes: • Trauma • Pathological causes( infections , tumors, osteoporosis )
Root nerve compression • A compressed nerve results when the nerve roots in the spinal cord are irritated or pinched. • Sciatica is the term usually used to describe the pain caused by compression of the spinal nerves, • Radiculopathy and radicular pain are the terms usually used by clinicians. • In the low back, the nerves most often compressed are at L5-S1. • The compression of nerve root causes pain to radiate into the buttocks and back of the thigh and calf, and may extend down to the foot.
Causes of root nerve compression • lumbar disc herniation: the most common cause of radiculopathy • spinal stenosis: a narrowing of the spaces within your spine • Spondylolithesis • forminal stenosis: (narrowing of the hole through which the spinal nerve exits due to bone spurs or arthritis) – more common in elderly adults • degenerative disorders.
Start to analyze of chief complain > Back pain !!! 1-Character • Aching throbbing pain = Inflammation • Intense sharp or stabbing = Radicular pain (e.g. Sciatica) 2-Time • Night, early morning = Inflammatory back pain • End of day, following activity = Mechanical pain
3- aggravating and relieving factor • Aggravated by activity and relieved by rest= Mechanical dysfunction. • Worse at rest and relieved by moderate activity = Inflammation. • Pain aggravated by standing or walking = Spondylolisthesis. • Pain aggravated by sitting and improved with standing = Discogenic problem (Degenerative Spinal Disorders).
4-Course: • Continuous pain, present day and night= neoplasia or infection. 5-history of psoriasis, diarrhea, penile discharge, eye trouble or severe pain in your joints: • Most common inflammatory disease that affect the back is spondyloarthropathies (Ankylosing Spondylitis)
6) Ask about constitutional symptoms: (Fever, weight loss ,night sweats and loss of appetite ) and history of malignancy = Spinal tumors 7) Related symptoms: such as -leg pain, weakness, and numbness; -Saddle anesthesia (S2-S5) -Urinary retention -fecal incontinence -CaudaEquina Syndrome!!!!! 8) Do you have any urinary symptoms? - UTI (Especially in pregnant women with low back pain)
Referred Pain • Pleuritic pain • Upper UTI / renal calculus • Abdominal aortic aneurysm • Uterine pathology (fibroids) • Irritable bowel (SI pain) • Hip pathology
RED FLAGS • Weight loss, fever, night sweats • History of malignancy • Acute onset in the elderly • Possible caudaequina syndrome • Immunosuppression (steroid) • Infection (current/recent) • Claudication or signs of peripheral ischaemia
A. Look : • Expose the trunk and lower limbs properly. • Any deformity, swelling, or skin changes. • Are shoulders & pelvis level. Gait: 1. Abnormal types: Antalgic, Trendelenberg, waddling. 2. Heel and toe walking: unable to heel walk= L4 weakness, unable to toe walk= S1 weakness . First: standing/walking position:
Examination B. Feel: • Palpate spinous processes for tenderness, steps or gaps. • Soft tissues: temperature, tenderness. C. Move: • Flexion. • Extension • Lateral bending • Rotation
Special test : • Adams Forward bending test Rib hump
Look: • Any muscle wasting in the lower limbs. • Feel: • Check for LLD • (ASIS to medial malleolus). Second: Supine position
Special tests: • Straight leg raising test (SLRT): • A positive test is reproduction of sciatica . • The pain is aggravated with dorsiflexion and relieved with knee flexion.
Neurologic examination: • Motor: • Hip flexion=L2 • Knee extension=L3 • Ankle dorsiflexion=L4 • EHL (Big Toe) =L5 • Ankle plantar flexion=S1
Sensory dermatomes. Tone normal, flaccid or rigid Reflexesknee & ankle jerks
Vascular examination: • Pedal pulses (dorsalispedis & posterior tibial). • Capillary refill (normal < 2 seconds)
Educate patient about the natural history of back pain • Ask about and address the patient’s concerns and goals • Maximizefunctional status. • Reliefthe pain. • Improveassociated symptoms, such as sleep or mood disturbances or fatigue. • Referral of complicated cases. • Prevention.
CaudaEquina Syndrome - EMERGENCY referral to ER. • Severe unremitting worsening of pain (at night and pain when laying down), consider infection/tumor – URGENT referral to ER for pain control – will need prompt investigation. • Significant trauma – consider fractures – check for instability and refer URGENTLY to spinal surgery. • Weight loss, fever, history of cancer/HIV – consider infection/tumor – refer URGENTLY for MRI Scan and to spinal surgery.
Use of IV drugs or steroids – consider infection /compression fracture – URGENT referral to spinal surgery. • Patient over 50 (if first ever episode of serious back pain) – refer SOON for prompt investigation/spinal surgery. • Widespread neurological signs – consider infection/tumor/neurological disease – refer SOON to neurology/spinal surgery/investigate further.
1- Lose weight: too much upper body weight can strain the lower back; you can use the healthy weight calculator to find out whether you need to lose weight or not. 2- Wear proper shoes: they can help reduce the pressure on your back. 3- Avoid sudden movements. 4- Try to reduce any stress, anxiety and tension, which can all cause or worsen back pain. 5- Stay active with regular exercise: Exercise is both an excellent way of preventing back pain and of reducing it, but should seek medical advice before starting an exercise programs if you've had back pain for six weeks or more.
6- Posture: How you sit, stand and lie down can have an important effect on your back. The following tips should help you maintain a good posture. 7- Standing: Stand upright, with your head facing forward and your back straight. Balance your weight evenly on both feet and keep your legs straight.
8- Sitting and driving: Make sure you sit upright with support in the small of your back. Your knees and hips should be level and your feet should be flat on the floor.
9- Sleeping: Your mattress should be firm enough to support your body while supporting the weight of your shoulders and buttocks, keeping your spine straight.
10- Lifting and carrying: One of the biggest causes of back injury, particularly at work, is lifting or handling objects incorrectly. • Think before you lift: • can you manage the lift? • Push rather than pull – if you have to move a heavy object across the floor, it is better to push it rather than pull it. .
Q1. The two most affected nerve roots in Radiculopathy? • L4 and L5. • L5 and S1. • S1 and S2. • L4 and S2.