Mood Killers: Hormones, Menopause, and Erectile Dysfunction
790 likes | 992 Vues
Mood Killers: Hormones, Menopause, and Erectile Dysfunction. Stacy Higgins, MD, FACP Emory University School of Medicine. Menopause. Definition. The permanent cessation of menses because of loss of ovarian follicular function A natural biologic process, not a disease!.

Mood Killers: Hormones, Menopause, and Erectile Dysfunction
E N D
Presentation Transcript
Mood Killers: Hormones, Menopause, and Erectile Dysfunction Stacy Higgins, MD, FACP Emory University School of Medicine
Definition • The permanent cessation of menses because of loss of ovarian follicular function • A natural biologic process, not a disease!
Why does it happen? • Aging of the female reproductive system starts at birth • Steady loss of eggs from either ovulation or atresia • Once last egg is depleted- menopause
Why so much attention? • Menopause affects every woman • Aging of the population means more women are postmenopausal than ever before • More postmenopausal women living beyond 65
Terminology • Pre-menopause • Peri-menopause • Post-menopause • Premature menopause • Premature ovarian failure • Induced menopause
Age at Menopause • Average age: 51.4 • (40-58) • Peri-menopause:47.5 • Lasts on average 4 years • No change in average age
When will it happen? • Later than average: • Multiparous • Increased BMI • Earlier than average: • Nulliparous • Medically treated depression • Seizure disorder • Smoking
Hormonal • Irregular menses • Decreased fertility • Osteoporosis
Vasomotor • Hot Flashes • Night Sweats • Sleep Disturbances
Urogenital Atrophy • Itching • Dryness • Bleeding • Urinary frequency and urgency • Urinary Incontinence
Skin Changes • Breast Atrophy • Skin Thinning • Decreased Elasticity • Thinning Hair
Psychological • Mood disturbance • Irritability • Fatigue • Memory loss • Depression
Sexual • Decreased Libido • Vaginal Dryness • Problems reaching orgasm • Dyspareunia
Diagnosis • Usually clinical diagnosis • FSH • Home Testing • What else might it be? • Pregnancy!! • Thyroid problems
Complications • Cardiovascular Disease • Osteoporosis • Urinary Incontinence • Weight Gain
Self-Care • Cool hot flashes • Decrease vaginal discomforts • Optimize your sleep • Strengthen your pelvic muscles • Eat well • Don’t smoke • Exercise regularly • Get regular checkups
Medical Symptom Management • Estrogen • Low-dose Antidepressants • Clonidine • Complementary Medicines
Systemic Estrogen • Most effective treatment option for relieving menopausal hot flashes • Take lowest dose needed to provide symptom relief • Weigh risk vs. benefit • Protects against osteoporosis • Increased risk of breast cancer, heart disease, stroke, and blood clots
Antidepressants • Venlafaxine (Effexor)- selective serotonin reuptake inhibitor (SSRIs) • Shown to decrease menopausal hot flashes • Other helpful SSRIs- fluoxetine (Prozac/Sarafem), paroxetine (Paxil), citalopram (Celexa) and sertraline (Zoloft)
Clonidine • Available as a pill or patch • Typically used to treat high blood pressure • May significantly reduce the frequency of hot flashes • Unpleasant side effects are common
Vaginal Estrogen • Relieves vaginal dryness • Can be administered using a vaginal tablet, ring or cream • Releases just a small amount of estrogen, which is absorbed by the vaginal tissue • Also helps relieve discomfort with intercourse and some urinary symptoms
Phytoestrogens • Two main types of phytoestrogens • Isoflavones: found in soybeans, chickpeas and other legumes • Lignans:occur in flaxseed, whole grains and some fruits and vegetables • Most studies have found them ineffective • Isoflavones have some weak estrogen-like effects
Black Cohosh • Used to treat hot flashes, night sweats, vaginal dryness, and other symptoms • Study results are mixed on whether black cohosh effectively relieves menopausal symptoms • Studies to date have been less than 6 months long, so long-term safety data are not currently available • Can cause headaches and stomach discomfort
Erectile Dysfunction • Inability to attain or maintain erection sufficiently firm to permit satisfactory sexual performance • Impotence is a broad term including problems of libido, erection and orgasm
How common is it? • Prevalence of 5% in men <40 years • Prevalence of 55-75% in men 75-80 years • Approximately 600,000 new cases of ED each year
Types of Dysfunction • Ability to obtain a full erection at some times (e.g. when asleep) • Obtaining erections which are either not rigid or full or lost rapidly
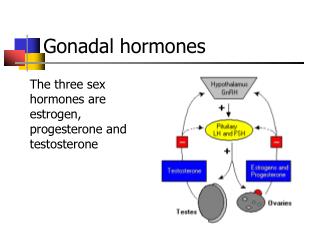
Physiology • Penis innervated by nerves • Blood vessels bring blood to the penis • Brain provides stimulation
How Does an Erection Happen? • Stimulation causes the brain to release chemicals • Chemicals bring message to nerves in the penis • Nerves tell penile blood vessels to relax • Blood flows into the penis • Pressure traps the blood, sustaining an erection
Causes • Physiologic • Impedence of blood entering and being retained in the penis • Psychologic • Erection or penetration fails due to thoughts or feelings rather than physical impossibility
Risk Factors • Vascular Disease is most common • Atherosclerosis • Diabetes • Hypertension • Cigarette smoking • Hypercholesterolemia
Risk Factors • Age • More time or more physical stimulation to achieve erection • More control over ejaculation, but flow is reduced • Tend not to be as hard, and the refractory period is prolonged • More likely to take medication that contributes to erectile dysfunction
Risk Factors • Medications • Antihypertensives (B-blockers, ACEI, Ca ch blockers, diuretics) • Antidepressants (TCAs, SSRIs) • Antipsychotics • Anticonvulsants • H2 receptor blockers • Statins and fibrates
Risk Factors • Endocrine Abnormalities • Hypogonadotropic hypogonadism • Hyperthyroidism • Hypothyroidism • Hyperprolactinemia