Endocrine Disorders: Nursing the client with Thyroid and Parathyroid dysfunction
840 likes | 1.53k Vues
Endocrine Disorders: Nursing the client with Thyroid and Parathyroid dysfunction. Jessica Doiron & Brandi Rambeau. Objectives. Overview of the Endocrine System Anatomy and Physiology of the Thyroid Functions Hormones Hypothyroidism and Hyperthyroidism

Endocrine Disorders: Nursing the client with Thyroid and Parathyroid dysfunction
E N D
Presentation Transcript
Endocrine Disorders: Nursing the client with Thyroid and Parathyroid dysfunction Jessica Doiron & Brandi Rambeau
Objectives • Overview of the Endocrine System • Anatomy and Physiology of the Thyroid Functions Hormones • Hypothyroidism and Hyperthyroidism • Hypoparathyroidism and Hyperparathyroidism • Thyroiditis • Thyroid Cancer Causes, Clinical Manifestations, Complications, Prevention, Medical Management and Nursing Care.
Thyroid Statistics • It is estimated that 200 million people in the world have some form of thyroid disease. • In Canada there is a staggering number of people affected. Recent studies indicate that 1 in 10 Canadians suffer from a thyroid condition of one type or another! Of those, as many as 50% are undiagnosed • Thyroid health affects all aspects of well being, both genders, all ages 4-7 times more common in women • The Thyroid Foundation of Canada in 1980 Early awareness essential to prevent complications Thyroid Foundation of Canada, 2013) (Thyroid Foundation of Canada, 2013).
Anatomy and Physiology of the Thyroid • Small butterfly-shaped gland • Location: lower neck anterior • to trachea • Blood flow to the thyroid is very high • Function: Hormones are essential for all growth and metabolism. • Gland regulates all body functions TFC, 2013
Thyroid Function and Dysfunction Various hormones and chemicals are responsible for normal thyroid function Key among them are: Thyroxine (T4) Triiodothyronine (T3) Calcitonin Iodine T3 + T4 known collectively as the THYROID HORMONE
The Thyroid HormoneT3 AND T4 • Amino acids containing iodine molecules • These hormones are essential for life and have many effects on body metabolism, growth, and development. Role of Iodine • Essential to the thyroid gland for synthesis of its hormones. • Major use of iodine in body is by the thyroid • If insufficient amounts = thyroid dysfunction
Actions of Thyroid Hormones Thyroid Hormones: T3 and T4 • Control cellular metabolic activity Increase metabolic processes by: increasing level of specific enzymes that contribute to oxygen consumption and altering the responsiveness of tissues to other hormones Helps the body convert food into energy and heat • The thyroid hormones influence cell replication and are important in brain development • Necessary for normal growth • Influence every major organ system • Increase body temperature
Calcitonin -Calcitonin is secreted in response to high plasma levels of calcium. It reduces the plasma level of calcium by increasing its deposition in bone -Calcitonin lowers blood calcium by: Inhibiting osteoclast activity in bones Inhibiting calcium absorption by the intestines Inhibiting renal tubular cell reabsorption of Ca, allowing it to be excreted in the urine
Iodine • Iodized salt • Salt from processed foods: bread, dairy products & processed meat • Saltwater fish and seafood • Not enough iodine = thyroid dysfunction • Concern with pregnant/lactating women: iodine requirements are higher (Zimmermann & Andersson, 2012).
Regulation of the Thyroid Hormone: The Hypothalamic-Pituitary Axis • Thyroid releasing hormone (TRH) from hypothalamus stimulates the pituitary gland to stimulate the thyroid stimulating hormone (TSH) • TSH stimulates the thyroid to produce T3 and T4 • If high levels of circulating T3 and T4 further TSH secretion is inhibited
Thyroid Function Tests • Laboratory measurements of thyroid hormones • Thyroid scanning • Biopsy • Ultrasonography
Thyroid Function Tests • Single, best measure of thyroid function is the serum TSH concentration • Measurement of TSH has a sensitivity and specificity of greater than 95%. • What can be measured? • TSH, FT4, T3 • The most widely used tests are • Serum immunoassay for TSH and serum free thyroxine (FT4).
Serum Free Thyroxine: FT4 • FT4 is the most common test used to confirm an abnormal TSH • Direct measure of free or unbound thyroxine • Methods include: • Dialysis method • Immunoassay technique: is less reliable in the measurement of FT4. It may be affected by medication, illness, or changes in protein binding. • Normal range: 10.3 – 35 pmol/L
Serum T3 and T4 • Measurement of total T3 or T4 includes protein-bound and free hormone levels that occur in response to TSH secretion • Serious systemic illnesses, medications and protein wasting r/t nephrosis and use of androgens may interfere with accurate test results. • Normal range T4: 65-138nmol/L • Normal range T3: 1.08-3.14nmol/L
Abnormal Thyroid Function • The state of normal thyroid function is called Euthyroidism. • Thyroid Disorders: can range from a small, harmless goiter (enlarged gland) that needs no treatment to life-threatening cancer. The main causes of thyroid disease are: • Hypothyroidism: too little thyroid hormone production • Think: depression of metabolic activity “slow down” • Hyperthyroidism: too much thyroid hormone production • Think: increased metabolic rate “speed up”
Hypothyroidism LOW
Thyroid Deficiency- Mild to Myxedema • Can affect all body functions: deficiency of thyroid hormone secretion and all metabolic processes SLOW DOWN. • Ranges from mild form (goiter) to advanced form and medical emergency: Myxedema
Clinical Manifestations Extreme fatigue and weakness Hair loss Weight gain Brittle nails Thick puffy or/Dry rough skin Numbness/tingling of fingers Husky/hoarse voice Menstrual disturbances Sensitivity to cold temperature Goitre/Atrophy of thyroid
Causes • #1 Hashimoto’s Thyroiditis:an autoimmune disease • that causes an inflammatory process of the thyroid gland • S&S = Goiter (enlarged thyroid gland) • Treatment of hyperthyroidism • Birth of a baby, born without a thyroid gland or a poorly functioning one (congenital hypothyroidism) • Surgical removal of the thyroid gland as a treatment for thyroid cancer. • Radiation to head or neck • Increased levels of iodine in the body • (Crawford & Harris, 2012)
Complications Goiter: enlarged thyroid Heart problems. Hypothyroidism may also be associated with an increased risk of heart disease. Infertility. Low levels of thyroid hormone can interfere with ovulation, which impairs fertility. Birth defects. Babies born to women with untreated thyroid disease may have a higher risk of birth defects than may babies born to healthy mothers (creitism) Myxedema. This rare, life-threatening condition is the result of long-term,undiagnosedhypothyroidism. (Crawford & Harris, 2012)
COMPLICATIONS: Myxedema • Rare, life-threatening condition • Result of long-term, undiagnosed hypothyroidism. • S&S: include intense cold intolerance and drowsiness followed by profound lethargy and unconsciousness. • Triggered by: Sedatives, infection or other stress on your body • Medical Emergency!
Medical Management • Goal restore normal metabolic state by replacing missing hormone. • Thyroid hormone replacement, daily for life • Synthetic thyroxine Synthroid or Levothroid • Periodic testing of TSH to assess treatment • Medication warnings: • Interaction of thyroid with other medications: may increase blood glucose levels and increase effect of digitalis, glycosides, anticoagulant medications. Increase risk osteoporosis. • In all pts with hypothyroidism, the effects of analgesic agents, sedatives and anaesthetic agents are prolonged • Particularly watch in the elderly. • (Dowben, Steele, Froelich, Vance, & Keltner, 2012).
Nursing Management • Modifying activity • Promote physical comfort • Provide emotional support • Monitor physical status • Assess cardiac function
Free floating thyroid hormones HYPERthyroidism
Hyperthyroidism Hyperthyroidism is the second most prevalent endocrine disorder, following diabetes mellitus It may appear after an infection, emotional shock, or stress. Other common causes include thyroiditis and excessive ingestion of thyroid hormone It affects women eight times more frequently than men Onset usually between second and fourth decades of life
Clinical Manifestations Nervousness Emotionally hyperexcitable Irritable Apprehensive Cannot sit quietly Palpitations Weight loss Intolerance to hot weather Thyroid enlargement (Goitre)
Hyperthyroidism: Clinical Manifestations continued Increased appetite and dietary intake Abnormal muscle fatigue and weakness Amenorrhea Tremor Exophthalmos Flushed skin (salmon color) Perspire unusually freely Changes in bowel function Systolic BP increase (but not diastolic) Atrial fibrillation may occur Osteoporosis and fracture associated with hyperthyroidism
Hyperthyroidism: Assessment and diagnosis Thyroid gland enlarged Thyroid is soft and may pulsate Thrill may be palpated A bruit may be heard over thyroid arteries Diagnosis of hyperthyroidism: based on symptoms and an increase in serum T4 and an increased radioactive iodine uptake
Hyperthyroidism: Management Depends on underlying cause Usually a combination of therapies Antithyroid agents Radioactive iodine Surgery
Hyperthyroidism: Management Radioactive Iodine Therapy -Goal is to destroy the overactive thyroid glands without affecting other radiosensitive tissues -Usually only one or two doses is required -Thyroid storm: monitor for signs and symptoms
Thyroid Storm: Management Immediate reduction of body temperature and HR Hypothermia blanket, ice packs ASA NOT used: it displaces the thyroid hormone from binding proteins and worsen hypermetabolism Humidified O2 IV fluids: containing dextrose to replace liver glycogen stores Hydrocortisone: tx shock or adrenal insufficiency Iodine: decrease output of T4 Propanolol, digitalis for severe cardiac symptoms
Hyperthyroidism: management Antithyroid medications: -to inhibit one or more stages in thyroid hormone synthesis -to reduce the amount of thyroid tissue= decreasing thyroid hormone production -block the action of iodine to prevent synthesis of thyroid hormones -monitor for S&S of agranulocytosis
Hyperthyroidism: nursing Dx Imbalanced nutrition Ineffective coping Low self-esteem Altered body temperature
Hyperthyroidism: Graves’ disease Occurs when antibodies such as thyroid-stimulating immunoglobulin and thyrotropinreceptor antibodies attack the thyroid gland, stimulating it to overproduce thyroxine (Weeks, 2005). Enlargement of thyroid gland or goiter Tx: medication, ablation therapy, surgery Ablation therapy: radioactive iodine is given in a small dose orally. The iodine collects in the thyroid gland: destroys overactive thyroid cells (Weeks, 2005).
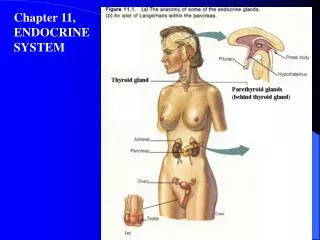
Parathyroid Dysfunction • 4 glands • Posterior to thyroid • Produces Parathyroid hormone (PTH) • Regulates calcium and phosophate metabolism 4 of them
HYPOparathyroidism Most common cause: Inadequate parathyroid hormone after interruption of blood supply or surgical removal of parathyroid gland. Hormone plays a key role in regulating and maintaining balance of body balance of two minerals: calcium and phosphorus
Pathophysiology Decrease Decrease Decrease • Lack of parathormone. • Decreased absorption of dietary Ca from gut • Decreased reabsorption of Ca by bone & renal tubules. • Decreased renal excretion of phosphate Overall: Low serum Ca levels results in hypocalcemia and high K serum levels results in hyperphosphatemia) Phosphate levels RISE Calcium levels FALL
Clinical Manifestations • Hypocalcemia TETANY (tremors, spasms, and uncoordinated contraction) • Tingling or burning (paresthesias) in your fingertips, toes and lips • Muscle aches or cramps affecting your legs, feet, abdomen or face • Fatigue or weakness • Painful menstruation • Patchy hair loss, such as thinning of your eyebrows • Dry, coarse skin • Brittle nails • Anxiety or nervousness • Headaches • Depression, mood swings • Memory problems
Assessment and Diagnosis Positive Trousseau’s sign Positive Chvostek sign Serum calcium levels of < 1.2-1.5 mmol/L Tetany develops Increased serum phosphate