Urinary System Diseases
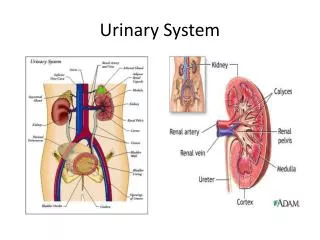
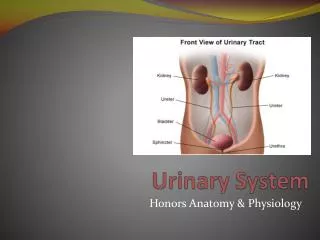
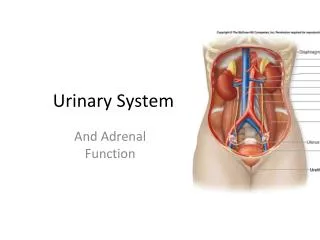
Urinary System Diseases. Pathophysiology. Review of Urinary Anatomy & Physiology. Located: Under back muscles Behind peritoneum Thus: retroperitoneal Below level of lowest ribs Right lower than left Adrenal gland on top of kidney Cortex Medulla Contains Pyramids & Papilla Pelvis

Urinary System Diseases
E N D
Presentation Transcript
Urinary System Diseases Pathophysiology
Review of Urinary Anatomy & Physiology • Located: • Under back muscles • Behind peritoneum • Thus: retroperitoneal • Below level of lowest ribs • Right lower than left • Adrenal gland on top of kidney • Cortex • Medulla • Contains Pyramids & Papilla • Pelvis • Calyx = division of pelvis • Pleural = calyces
Bladder • Lined with transitional epithelium • Can stretch • Lined with rugae • Trigone • On posterior wall • Where ureters & urethra open • Rigid area with NO rugae • Micturition (voiding, urination) • Internal urinarysphincter • Involuntary • External urinary sphincter • Voluntary • Stretch receptors in bladder wall
Nephron = functional unit • Consists of: • Renal Corpuscle • Renal Tubules • Renal Corpuscle contains: • Bowman’s capsule • Part of collecting system • Glomerulus • Afferent arteriole • Efferent arteriole • Renal Tubules 1. Proximal convoluted tubule 2. Loop of Henle 3. Distal convoluted tubule 4. Collecting tubule
Key point: The cortex contains all the structures of the nephron The medulla contains only the collecting ducts & the loop of Henle
Functions of the kidney Removes nitrogenous wastes Urea Uric acid Creatinine Ammonia Maintains homeostasis Fluid balance Electrolyte balance Acid-base balance Excretory Organ Via blood filtration & formation of urine Regulation of Blood Pressure Juxtaglomerular apparatus RAA system Renin Angiotensin Aldosterone Urine formation Filtration Occurs in renal corpuscle Reabsorption Occurs in proximal convoluted tubule Also occurs in distal convoluted tubule It takes things back into blood Secretion Occurs in distal convoluted tubule Blood gives things up to the urine Concentration Occurs in collecting tubules See next slide
Some Key Points of Renal Physiology • Nitrogenous wastes primarily come from breakdown of proteins • Aging & renal function • By age 35, one begins to lose nephrons • By age 80, one has approx. 30% reduction in nephron capacity • GFR = glomerular filtration rate • Normal = 125cc/min (7500cc/hour) • 99% of filtered product is reabsorbed • Normal urine output = 60cc/hour (1500cc/day) • All along the duct system water is reabsorbed • Includes the prox. conv. tubule, loop of Henle, distal conv. Tubule, & collecting tubule • Sodium follows water • Key elements involved in each process • Reabsorption = H2O(Na), proteins (amino acids), & sugars(glucose) • Secretion = ions(K+), drugs, ammonia • Concentration = more reabsorption of H2O
2 key factors determine volume of urine produces • Glomerular filtration rate (GFR) • Determined by the unique arrangment of blood vessels • Hormonal secretion • Determined by fluid & electrolyte balance
Unique arrangment of blood vessels • Afferent arteriole -----to----capillary bed-----to----efferent arteriole -----to-----capillary bed ----to---- veins • First capillary bed = glomerular capillaries • Second capillary bed = peritubular capillaries • Purpose of this = to control the pressure in the glomerular capillaries & consequently the glomerular filtration pressure • 3 factors control this: • (1) autoregulation • Local feedback from muscle tension in afferent arteriole • Local feedback from DCT at JGA • Mediated via endothelial • secretions of glomerular capillaries • (2) sympathetic nervous system • (3) renin Volume of urine also controlled by glomerular filtration rate
B = increase fluid volume; overhydration; high output heart failure • C = kidney pathology • D = hypertension; arteriolar spasm
Hormones help control the volume of urine via fluid & electrolyte balance • The concentration factor essentially deals with urine volume • Usually more the volume = more the dilution [a direct proportion] 1. Aldosterone • From adrenal cortex • Works on distal convoluted tubule • Causes H2O & Na+ retention 2. Atrial natriuretic hormone(ANH) • From atrial wall of heart • Works on distal convoluted tubule • Works in opposition to aldosterone • Causes H2O & Na+ loss 3. Antidiuretic hormone • From posterior pituitary • Works on collecting tubules • Causes reabsorption of H2O (Na+ goes with it)
1. Physical Characteristics &Measurements appearance color odor volume specific gravity 2. Chemical Measurements pH protein; glucose ketones bilirubin; urobilinogen leukocytes; nitrite blood 3. Microscopic cells (wbc, rbc, sperm) casts crystals bacteria 4. Detection of Bacteriuria nitrite test qualitative or screening test C & S Colony Count, if done, make this a quantitative test NOTE: Step 4, qualitatively, is doneas part of step 2 Diagnostic Tests - Urinalysis
Appearance Clear = normal Cloudy = ? Infection If sediment = kidney disease Dark = ?blood, ?bilirubin, ?concentrated Color Urochrome pigment = yellow comes from breakdown of hemoglobin Concentration More Concentrated = Deeper Yellow Change of Color From: Meds Vitamin = yellow Diseases Blood = red-brown Liver = Orange Foods Rhubarb = red-brown Odor Normal = ammonia-like smell from breakdown of urea Unpleasant = ? infection Quantity Average per 24 hours = 1500 cc 60 cc per hour GFR = 125 cc/min Thus, 7500 cc/ hour Urine Made Per Hour = 60 cc Urine GFR Per Hour = 7500 cc KEY: 1 % of filteredurineremains urine; 99 % becomes reabsorbed back into blood Oliguria = 100 - 400 cc per day Anuria = less than 100 cc per day Polyuria = diabetes, nerves, diuretics
Specific Gravity Determines Concentration Compares Test Liquid to H2O Normal = 1010 - 1030 First AM Specimen = > 1020 In many kidney diseases, one loses the ability to concentrate urine 3 ways to do it: 1. Reagent Strip 2. Refractometer 3. Urinometer pH Determines Acidity or Alkalinity Normal = 6.0 Range = 4.5 - 8.0 Acidity example = diabetes Alkaline example = UTI Protein OK to have a Trace in the urine Benign Conditions: exercise exposure to cold protein consumption Generally Means Kidney Disease Glucose Will only be in urine if exceed Renal Threshold (160 - 180 mg/dl) Ketone (note Acetone is a Ketone) Ketones are products of Fat Metabolism If cant breakdown Sugars for energy, the body will begin using Fat Seen in: Uncontrolled Diabetes Starvation Hi-Fat Diet
Bilirubin & Urobilinogen Formation When used-up RBC’s are broken down by R-E System, a by-product is Bilirubin Bilirubin removed from blood by liver & excreted into intestine Bacteria in intestine convert Bilirubin into Urobilinogen Some Urobilinogen reabsorbed into blood Of this amount reabsorbed some my be normally passed in urine Bilirubin Normally None in Urine Found in urine if it can’t get from the liver into G-I tract From Obstruction of Bile Ducts Found in urine if have: Liver Disease (hepatitis) Blood Disease (hemolysis) Urobilinogen generally follows whatever happens to bilirubin may get none in urine if on antibiotics (destruction of gut flora) usually get small amount in urine Blood None is normal But may see some if female is menstruating Leukocytes from inflammation of kidney or lower G-U tract Nitrites screening test for bacteriuria bacteria convert nitrate to nitrite
Other Diagnostic Tests • Blood tests • BUN / creatinine • CBC ------ anemia if decreased EPO production • Renin • Antistreptolysin titers • Urine culture & sensitivity (C&S) • Include colony count • Imaging • IVP • Retrograde pyelography • CAT/ MRI • Surgical procedures • Cystoscopy • Biopsy
Urinary Tract Disordersoverall outline • Incontinence & retention • UTI’s • Inflammatory disorders • Nephrotic syndrome • Urinary tract obstruction • Stones • Hydronephrosis • Tumors • Renal cell carcinoma • Bladder cancer • Congenital disorders • Polycystic kidneys • Wilm’s tumor (nephroblastoma) • Renal failure • Acute • Chronic • Dialysis
Urinary Incontinence Loss of voluntary control of bladder Frequently called “neurogenic bladder” Many causes Enuresis = involuntary control after age 4 or 5 Types: Stress Urge Overflow Urinary retention Called “residual urine” Causes : Anatomical defects Neurogenic defects Treated with “catheterization” Foley French Incontinence, retention, & catheters
Urinary Tract Infections Urethritis; Cystitis; Pyelonephritis • Etiology • Ascending infection ----- women > men • Prostatic hypertrophy with urinary retention • Incomplete emptying of bladder with urinary stasis • Pregnancy associated with stasis • Blood borne pathogens • Pathophysiology of UTI’s ----- see next slide • Dx • Dysuria, urgency, & nocturia • Systemically get fever & malaise • CVA tenderness in pyelonephritis • Note glomerulonephritis is vastly different with regards etiology & pathophysiology
Note etiologies • Inflammation of mucosa • Trauma of mucosa • Obstruction • Vesicoureteral reflux • Immobility • Blood-borne pathogens • TB • HIV • Septicemia
Glomerulonephritis Acute Sx = proteinuria, edema, oliguria Etiol = 1-2 weeks post strept infect. Chronic Etiol = autoimmune disease e.g. lupus, diabetes, hepatitis C Can lead to irreversible kidney damage Inflammatory disorders(1) glomerulonephritis (2) nephrotic syndrome
Nephrotic Syndrome • Glomerular disorder where one loses the capacity to retain protein, especially albumin • Sx • severe edema (anasarca) • * can get skin breakdown since impaired arterial flow • proteinuria • hypoalbuminemia • oliguria • Etiol: • Toxic agents (lead, mercury) • Toxic drugs (aminoglycosides) • Diseases (diabetes, lupus • Key = any significant problem with • glomerulus can lead • to nephrotic syndrome
Tumors Note that primary symptom = hematuria Renal Cell Ca = most common, unilateral, adeno Ca from tubular epithelium See picture Bladder Ca = usually from transitional epithelium Neurogenic bladder Renal Calculi Etiology: Calcium, Uric acid, Urine crystals Symptoms: renal colic, N&V, chills, fever Risk factors: prolong dehydration, prolong immobilization, infection Treatment: surgery,lithotripsy Anomalies Strictures Kinks Ptosis Pelvic kidney Obstructive Disorders
These result in: • Hydronephrosis • Hydroureter • If these conditions exist longer than 2 months get destruction of kidney Major sites of urinary tract obstruction
Congenital Diseases • Vesicoureteral reflux • Due to ectopic insertion of ureter into bladder. If far away from trigone, do not get adequate compression of ureter when voiding & get reflux • Incidence: 1/1000 • If one gets it each sibling(to be) has 50% incidence • Girls> boys; 10:1 ratio • Ectopic kidney • May get kinking of ureter • Usually in pelvis • Asymptomatic • Renal agenesis • Usually unilateral & left kidney • 2 types: (1) occurs randomly (2) genetic • Asymptomatic • Remaining kidney becomes large since compensatory hypertrophy
Congenital Diseases (cont) • Polycystic kidney (2 types • In adults (see picture) • Genetic etiol ----- autosomal dominant • Clinically seen in adults • Between age 30 – 40 one begins to get renal failure • Tx = transplant • In children • Genetic etiol --- autosomal recessive • Manifest at birth; usually fatal or infant stillborn • Rare • Wilm’s tumor (nephroblastoma) • Most common tumor of children; usually unilateral • Etiol = autosomal recessive (on chromosome 11) • Manifests between age 2 – 5 years & presents as abdominal mass • May produce hypertension • 5 year survival = 90%
Acute renal failure Abrupt decrease in renal function Nitrogenous wastes accumulate Usually reversible Sx: Oliguria Drowsiness Altered levels of consciousness Etiol: Glomerular disease Severe pyelonephritis Nephrotoxins that damages tubular epithelium Ischemic causes shock ATN (acute tubular necrosis) e.g. burns(hgb accumulates) e.g. trauma (myoglobin accumulates) Renal Failure
Chronic Renal Failure • Get slow progressive loss of neurons • Usually irreversible • Course = gradual • Etiol: • Vascular disease • e.g. hypertension • Disease callednephrosclerosis • Glomerular disease • e.g. diabetes • Tubular disease • e.g. toxins Hypertension & the kidneys
2 types: Hemodialysis Peritoneal dialysis Mechanism Simple diffusion for wastes & electrolytes Osmosis for water balance Dialysis in renal failure