Urinary System
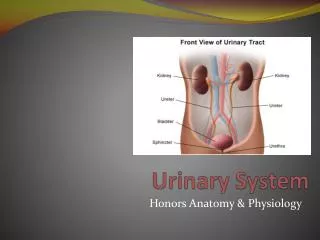
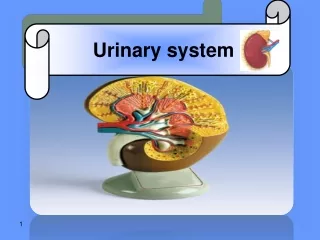
Urinary System. Chapter 13 A&P1 Tutor: Eleshia Howell. The urinary system is the main excretory system, removing the majority of physiological wastes. It consists of the following structures: Kidneys x 2 Ureters x 2 Urinary bladder Urethra

Urinary System
E N D
Presentation Transcript
Urinary System Chapter 13 A&P1 Tutor: Eleshia Howell (c)Eleshia Howell, 2012.
The urinary system is the main excretory system, removing the majority of physiological wastes. • It consists of the following structures: • Kidneys x 2 • Ureters x 2 • Urinary bladder • Urethra • Apart from the elimination of wastes, the kidneys also play a vital role in several other homeostatic functions, eg BP, blood volume, electrolyte balance, blood pH, water balance. (c)Eleshia Howell, 2012.
The kidneys produce urine that contains metabolic waste products, including the nitrogenous compounds Urea and Uric acid, excess ions and some drugs. • Urine is stored in the bladder and excreted by the process of micturition via the urethra. (c)Eleshia Howell, 2012.
Kidneys • Lie on the posterior abdominal wall, one on each side of the vertebral column, behind the peritoneum and below the diaphragm. • The extend in length from T12 – L3, receiving some protection superiorly from the ribcage. • The right kidney is usually slightly lower than the left (displaced by large Liver above). • They are ‘bean’ shaped, weigh approx 150g and are embedded in a mass of fat which helps to protect them and hold them in position. (c)Eleshia Howell, 2012.
A sheath of fibrous connective tissue, the renal fascia, encloses both the kidney and the renal fat. • The adrenal glands sit atop the kidneys; affect kidney function by the secretion of hormone Aldosterone which helps to regulate the osmolarity of blood plasma. • Viewed with the naked eye, there are 3 distinct areas of tissue seen in the kidney. • Outer fibrous capsule • Cortex – reddish-brown layer • Medulla – innermost layer, pale conical shaped striations known as renal pyramids (c)Eleshia Howell, 2012.
A hilum is present on the concave medial border, where the renal blood and lymph vessels, the ureter and nerves enter. • The renal pelvis is the funnel-shaped structure that collects urine formed by the kidney. The walls of the pelvis contain smooth muscle are lined with transitional epithelial cells. Intrinsic propulsion of urine via the calyces (plural of calyx) to the renal pelvis then on to the ureter occurs without nervous system control. (c)Eleshia Howell, 2012.
p331 (c)Eleshia Howell, 2012.
On a microscopic level, the kidney is composed of about 1-2million functional units called nephrons, and a smaller number of collecting ducts. • The collecting ducts transport urine through the pyramids to the calyces and renal pelvis, giving the pyramids their striped appearance. • A small amount connective tissue, containing blood vessels, nerves and lymph vessels supports the collecting ducts. (c)Eleshia Howell, 2012.
The Nephron • Consists of a tubule, closed at one end; the other end opens into a collecting tubule. • The closed end forms a cup-shaped structure known as the glomerular capsule or Bowman’s capsule, which almost completely encloses a network of tiny arterial capillaries ~ the Glomerulus. • The rest of the nephron is about 3cm long and is described in 3 parts... (c)Eleshia Howell, 2012.
Proximal convoluted tubule • Medullary loop (Loop of Henle) • Distal convoluted tubule (which leads into collecting duct). • The collecting ducts unite, forming larger ducts that empty into the minor Calyx (c)Eleshia Howell, 2012.
A Nephron (simple) (c)Eleshia Howell, 2012.
The kidneys receive about 20% of the cardiac output • After entering the kidney at the hilum the renal artery divides into smaller arteries & arterioles. In the cortex, an afferent arteriole enters each glomerular capsule and then subdivides into a cluster of tine arterial capillaries, forming the glomerulus. • Between these capillary loops are modified connective tissue cells, called mesangial cells, which are capable of a number of functions. (c)Eleshia Howell, 2012.
Location of Mesangial cells (c)Eleshia Howell, 2012.
The blood vessel leading away from the glomerulus is the efferent arteriole. • The AFFERENT vessel has a larger diameter to increase the pressure inside the glomerulus, driving filtration across the capillary walls. • The efferent vessel divides into a second set of capillary network, wrapping around the renal tubules to maintain a supply of oxygen and nutrients to the local tissue, as well as removing waste products. (c)Eleshia Howell, 2012.
The walls of the glomerulus and its capsule are a single layer of flattened epithelial cells, with the glomerular walls being more permeable than those of other capillaries. • The remainder of the nephron and collecting duct are formed by single layer of simple squamous epithelium. • Blood vessels of the kidneys have both sympathetic and parasympathetic nerve supply, controlling renal blood vessel diameter and blood flow (independently of autoregulation*) (c)Eleshia Howell, 2012.
Functions of the Kidney • Formation of Urine. The composition of urine reflects the exchange of substances between the nephron and blood in the renal capillaries. Waste products of protein metabolism are excreted, electrolyte levels are controlled and pH (acid-base balance) is maintained by the excretion of hydrogen ions. (c)Eleshia Howell, 2012.
There are 3 processes involved in the formation of urine: • Filtration – occurs in the semipermeable walls of the glomerulus and capsule. Some substances pass through while others remain in the capillaries. Filtration transpires due to the difference in hydrostatic pressure between the blood in glomerulus (higher) and osmostic pressure of the blood in the capsule (lower). Approx 125ml / min or 180L a day is filtered by both kidneys, but less than 1% (1-1.5L) is excreted as urine. (c)Eleshia Howell, 2012.
p334 (c)Eleshia Howell, 2012.
Renal blood flow is protected by a mechanism called autoregulation, whereby renal blood flow is maintained at a constant pressure across a wide range of systolic blood pressures (from 80-200mmHg). It operates independently from ANS control; therefore only inherent changes to blood pressure in the renal arteries will have an impact, eg fluctuating levels of metabolites (such as prostaglandin). In severe shock, when systolic pressure falls below 80- autoregulation fails and renal blood flow & hydrostatic pressure decreases, impairing filtration in nephrons. (c)Eleshia Howell, 2012.
Selective Reabsorption Most reasborption from the filtrate back into the blood takes place in the proximal convoluted tubule (which is lined with microvilli). Materials essential to the body are reabsorbed here (water, electrolytes, glucose). Some reabsorption is passive and some requires active transport. Only 60-70% of filtrate reaches the loop of nephron where most of the water, sodium & chloride is absorbed, leaving approx 15-20% left to reach the distal convoluting tubule. (c)Eleshia Howell, 2012.
The kidney’s maximum capacity for reabsorption of a substance is known as the renal threshold. This eventuates if all the mechanisms for transport are ‘occupied’ or the tubules are overloaded. • The renal threshold for substances varies according to body need at any particular time and in some cases, is regulated by hormones • Parathyroid hormone – calcium, phosphate • Anti-diuretic hormone – increases water reabsorption • Aldosterone – increases reabsorption of water & sodium, and excretion of potassium • AtrialNatriuretic Peptide – decreases absorption of water & sodium (c)Eleshia Howell, 2012.
Tubular Secretion Substances not required and foreign materials, such as drugs, may not be cleared from the blood by filtration (because of the short time it remains in the glomerulus) so are cleared by secretion from the peritubular capillaries into the convoluted tubuled for excretion in the urine. (c)Eleshia Howell, 2012.
p336 Summary of urine formation (c)Eleshia Howell, 2012.
Composition of Urine: • Water 96% • Urea 2% • Uric acid • Creatinine • Ammonia • Sodium • Potassium • Chlorides • Phosphates • Sulphates • Oxalates 2% (c)Eleshia Howell, 2012.
Urine should be clear (not cloudy) and amber in colour • A healthy adult passes 1000 – 1500ml / day • Specific gravity is normally between 1020 – 1030 ~ this will vary according to fluid intake (as will the colour & amount). • Urine production is decreased during sleep and exercise. (c)Eleshia Howell, 2012.
Kidney Function cont’d • Water Balance & Urine Output The source of most body water is dietary food & fluid, with only a small amount of ‘metabolic water’ produced during metabolic processes. Water is excreted in urine, air, faeces and sweat. The balance between fluid intake and output is controlled by the kidneys. The minimum amount of urinary output (required to excrete body waste) is 500ml / day. (c)Eleshia Howell, 2012.
Urinary volume in excess of the minimum is controlled mainly by ADH released from the posterior pituitary. • Sensory nerve cells (osmoreceptors) in the hypothalamus, when stimulated, refer impulses to the posterior pituitary to release ADH, ie if the blood is becoming more concentrated, ADH output is increased, increasing the reabsorption of water from the distal convoluted tubules and collecting ducts. This negative feedback mechanism maintains normal blood osmotic pressure (and therefore sodium & water concentrations). (c)Eleshia Howell, 2012.
Electrolyte Balance An electrolyte is any substance containing free ions that make the substance electrically conductive. The primary ions of electrolytes are sodium (Na+), potassium (K+), calcium (Ca2+), magnesium (Mg2+), chloride (Cl−), hydrogen phosphate (HPO42−), and hydrogen carbonate (HCO3−). The electric charge symbols of plus (+) and minus (−) indicate that the substance is ionic in nature and has an imbalanced distribution of electrons. Sodium is the main electrolyte found in extracellular fluid and is involved in fluid balance and blood pressure control. (c)Eleshia Howell, 2012.
Our bodies require a subtle and complex electrolyte balance between the intracellular and extracellular environment. In particular, the maintenance of precise osmotic gradients of electrolytes is important. Such gradients affect and regulate the hydration of the body as well as blood pH, and are critical for nerve and muscle function. Various feedback mechanisms exist to keep the concentrations of different electrolytes under tight control. (c)Eleshia Howell, 2012.
Both muscle tissue and neurons are considered electric tissues of the body. Muscles and neurons are activated by electrolyte activity between the interstitial fluid, and intracellular fluid. Electrolytes may enter or leave the cell membrane through specialized protein structures embedded in the plasma membrane called ion channels. eg, muscle contraction is dependent upon the presence of calcium (Ca2+), sodium (Na+), and potassium (K+). Without sufficient levels of these key electrolytes, muscle weakness or severe muscle contractions may occur. (c)Eleshia Howell, 2012.
Electrolyte balance is maintained by oral, or in emergencies, intravenous (IV) intake of electrolyte-containing substances, and is regulated by hormones, generally with the kidneys flushing out excess levels. Electrolyte homeostasis is regulated by hormones such as antidiuretic hormone, aldosterone and parathyroid hormone. Serious electrolyte disturbances, such as dehydration and overhydration, may lead to cardiac and neurological complications and, unless they are rapidly resolved, will result in a medical emergency. (c)Eleshia Howell, 2012.
Changes in the concentration of electrolytes in the body fluids may be due to changes in: • Body water content • Electrolyte levels Renin-angiotensin-aldosterone System: • Sodium is a normal constituent of urine and the amount excreted is regulated by the hormone Aldosterone (secreted by adrenal cortex). • Cells in the afferent arteriole of the nephron release the enzyme Renin in response to sympathetic stimulation, low blood volume or low arterial blood pressure. (c)Eleshia Howell, 2012.
Renin converts the plasma protein Angiotensin (produced by the liver) to angiotensin1. • ACE (angiotensin converting enzyme) secreted by the lungs & proximal convoluting tubules, converts angio1 to angio2 which is a powerful vasoconstrictor and increases BP. Water and sodium absorption is increased, in turn increasing blood volume. This, then, leads to reduced renin secretion (negative feedback) and balance is restored. (c)Eleshia Howell, 2012.
Calcium balance Regulation of calcium levels is achieved by co-ordinated secretion of parathyroid hormone and calcitonin (thyroid). The distal collecting tubules reabsorb more calcium in response to PTH and reabsorb less in response to calcitonin secretion. (c)Eleshia Howell, 2012.
pH Balance The cells of the proximal convoluted tubules secrete hydrogen ions to maintain normal blood pH. In the filtrate they combine with a number of buffers, which neutralise highly acidic / alkaline substances and excrete excess ions into the urine. The normal pH of urine is between 4.5 - 8. A diet high in animal proteins tends to produce more acidic urine (low pH) than vegetarians. (c)Eleshia Howell, 2012.
Ureters • These are the tubes that carry urine from the kidneys to the urinary bladder • They are approx 25-30cms long, 3mm diameter. • Each ureter is continuous with the renal pelvis of the kidney it extends from, passing down through the abdominal cavity, behind the peritoneum, in front of the psoas muscle before passing obliquely through the posterior wall of the bladder. (c)Eleshia Howell, 2012.
p338 (c)Eleshia Howell, 2012.
The entry of the ureters into the posterior wall of the bladder helps to prevent backflow of urine ~ the pressure of accumulated urine in the bladder compresses the opening of the ureters, as does the muscular contraction of the bladder during micturition. • The walls of the ureters consist of 3 layers of tissue: • Outer fibrous layer, continuous with capsule of kidney • Middle smooth muscle layer • Inner mucosal layer composed of transitional epithelium. (c)Eleshia Howell, 2012.
Function of Ureters: • Propulsion of urine from kidneys to bladder by peristaltic contraction of smooth muscle layer. This is an intrinsic property, not under autonomic control. Peristalsis originates from a ‘pacemaker’ in the minor calyx of the kidney, producing several waves a minute, sending little spurts of urine into the bladder. (c)Eleshia Howell, 2012.
Urinary Bladder • The bladder is roughly pear-shaped, but becomes more oval as it fills with urine, distending into the abdominal cavity as it fills to capacity. • The bladder opens into the urethra at its lowest point, the neck. • The peritoneum covers only the superior surface, but in females it surrounds the uterus posteriorly; in males it surrounds the rectum. (c)Eleshia Howell, 2012.
The bladder wall is composed of 3 layers: • Outer loose connective tissue, containing blood & lymph vessels & nerves • Middle interlacing smooth muscle & elastic tissue • Inner mucosal layer • When empty, the inner lining is arranged in folds (rugae) which expand as bladder fills with urine. • At 300-400ml we become aware of the need to urinate.Total capacity is approx 600ml. • Internal urethral sphincter controls flow of urine from the bladder (involuntary control). (c)Eleshia Howell, 2012.
p340 (c)Eleshia Howell, 2012.
Urethra • A canal extending from the neck of the bladder to the exterior of the body (external urethral orifice – voluntary control) • Longer in males than females • In males has dual function with reproductive system. • In females, the urethra extends down behind the symphysis pubis and exits superior to the vaginal opening. (c)Eleshia Howell, 2012.
Micturition • When 300-400ml of urine accumulates in the bladder, afferent autonomic nerve fibres sensitive to stretch are stimulated. • In infants, this initiates the spinal reflex, causing instant urination. • When nervous system is fully developed, the micturition reflex is stimulated but sensory impulses also reach the brain, creating an awareness to urinate. By learned and conscious effort, the external urethral sphincter & pelvic floor muscles can inhibit micturition. (c)Eleshia Howell, 2012.
Over-distension of the bladder is painful and can be overridden by involuntary relaxation of the external urethral sphincter, allowing a small amount of urine to escape the bladder. • Involuntary loss of urine is known as incontinence. (c)Eleshia Howell, 2012.
Pathologies of the Kidneys • The kidneys have considerable functional reserve meaning that impairment of renal function does not become evident until the equivalent of more than one kidney is lost. Hence the ability for a healthy person to be able to donate one of their kidneys. (c)Eleshia Howell, 2012.
Terminology: • Oliguria – less than 400ml/day urinary output • Haematuria – presence of blood in urine • Proteinuria – presence of protein in urine • Anuria – absence of urine • Dysuria – pain on passing urine • Glycosuria – presence of sugar in urine • Ketonuria – presence of ketones in urine • Nocturia – passing urine during the night • Polyuria – unusually large amounts of urine • Incontinence – involuntary loss of urine • Frequency of micturition – sml amounts often (c)Eleshia Howell, 2012.
GLOMERULONEPHRITIS: • Several types, not all display inflammatory properties. • In many cases, immune complexes damage the glomeruli (the antigen-antibody complex has formed in the kidney and lodged in walls of glomerulus, causing inflammatory response, impairing function). • Extent may be diffuse or focal • May also be caused by infection, systemic conditions (eg Lupus, endocarditis), medication, disease. (c)Eleshia Howell, 2012.