Download
1 / 18
180 likes | 202 Vues
This course explores the implementation of cost effectiveness in the appraisal process, focusing on understanding the threshold value and how to weight cost effectiveness with other considerations. It also examines the variable nature of the threshold and the impact of burden of disease on decision making.

E N D
How to weight cost effectiveness in appraisal NVTAG / CVZ course:The appraisal process, work in progress 22th of April 2009 Jan van Busschbach
Context investigation CVZ • Cost effectiveness is considered in all new reimbursement application • Cost effectiveness is an important aspect in the appraisal • How to implement cost effectiveness in appraisal?
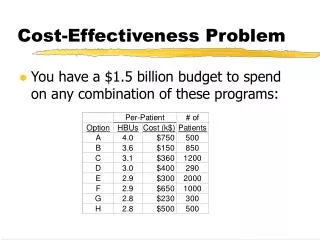
Two research questions: • What is a “good” and what a “bad” cost effectiveness? • What is the threshold value? • In terms of costs per QALY • How does one weight cost effectiveness with other considerations?
What is the threshold value? • Should there be a threshold value? • If there was one: what is the point in weighting with other arguments? • A threshold provokes strategic behavior • Is there a normative paradigm (theory), that provides such threshold? • The need for a threshold is pragmatic • It helps to chose between good and bad • Its value is historical determined
Threshold most likely a range • A range like in England and Scotland • £ 20.000 - £ 30.000 • But higher values are possible • As defined by RvZ maximum € 80.000 per QALY • In de media € 80.000 seem threshold • But much lower values also possible
Cost effectiveness in practice • Threshold might stand for average cost effectiveness in practice • Average cost per QALY • Meerding et al, 2007 • Cardiovascular diseases: € 2.000 to € 5.000 per QALY • Oncology: €16.000 tot € 18.000 per QALY • In practice: • A range • Averages cost effectiveness is lower than used in most debates about the threshold
Conclusion research question 1 • What is a “good” and what a “bad” cost effectiveness? • What is the threshold value? • In terms of costs per QALY • There is no empirically or theoretically fixed value • More likely: a range (of thresholds) • Other variables determine good or bad cost effectiveness
A variable threshold • Research question 2 • How does one weight cost effectiveness with other considerations? • Same question as: • Is the threshold variable? • If so: which variables have an influence? • For instance: • does disease burden interacts with threshold value? • CvZ models 2001, RvZ model 2006, 2007
A variable thresholdThe RvZ model: interaction with burden Costs per QALY Burden of Disease
Interaction with Burden • Burden of disease most often discussed • As candidate to alter decision making • To weight cost effectiveness • Know as the equity debate • Maximize average population health… • Without looking at burden of disease • Focus on the worse of…. • Without looking at the average population health • Interaction is intermediate position in debate
Methodology issues • How to measure burden? • What should be the form of the curve? Cost per QALY Burden of disease
But we do know… • The function is continuously ascending • Burden can be measured • Next presentation: Elly Stolk • We can deduct the curve from research • Population preferences • The appraisal committee
Other argument than burden might be also be relevant Examples are rarity (orphan drugs), budget impact, live style etc. Some might increase the threshold, some might lower it… Next to burden….
Increasing or lowering the threshold • Increasing • Burden • Rarity (orphan drugs) • Relates to much informal care • Risks for others • Lowering • Limited relation to domain of health care • High budget impact • High future medical costs • Unsuitable for insurance because of high incidence • Unsuitable for insurance because of autonomy patient
Increasing threshold, and critics Burden But lower population health… Rarity (orphan drugs) Cause of disease becomes more important that burden and effectiveness… Does not make much sense from epidemiology point of view Relates to much informal care Could be include in the CE-ratio… Risks for others Could be include in the CE-ratio…
Lowering the threshold, and critics Limited relation to domain of health care What is the domain of health care...? High budget impact Focus on costs, not on cost effectiveness High future medical costs Could be include in the CE-ratio… Unsuitable for insurance because of high incidence Might cause people to avoid health care Unsuitable for insurance because of autonomy patient Might cause people to avoid health care
Conclusions There does not seem to be a fixed threshold Many factors might alter threshold Burden of disease is best described Decisions of the appraisal committee will reveal trade-off between cost effectiveness and other arguments