Download
1 / 104
1.04k likes | 1.2k Vues
T. Lau, MD, FRCPC [psych], MSc., Assistant Professor, Faculty of Medicine, UNIVERSITY OF OTTAWA Royal Ottawa Mental Health Centre Geriatrics. Updated Jan 2008. Anxiety SAD, SP, GAD, PTSD, OCD, Panic+/-A, Separation AD Associated w depression / psychosis Somatoform / Dissociative disorders

E N D
T. Lau, MD, FRCPC [psych], MSc., Assistant Professor, Faculty of Medicine, UNIVERSITY OF OTTAWA Royal Ottawa Mental Health Centre Geriatrics • Updated Jan 2008
Anxiety • SAD, SP, GAD, PTSD, OCD, Panic+/-A, Separation AD • Associated w depression / psychosis • Somatoform / Dissociative disorders • PD • S-GMC • Personality • Traits and disorders • 3 Clusters • MAD • BAD • SAD • Different Domains • Extroversion, introversion • Harm avoidance-novelty seeking • Substance • ETOH • Uppers • Downers • Mixed • Rx • Mood • MDD • BAD • Dysthymia • Cycothymia • Adjustment • Bereavement • SCZ-A/SCZ • Substance-GMC • PD • S-GMC • Psychosis • Mood D/O (MDD or BAD) • SCZ • BPE • Dissociative D/O • Delusional disorder • Delirium • PD • S-GMC Cognition: Delirium, Dementia, NOS, Psychosis, Dissociative, Mood or anxiety d/o [performance], MR-PDD, S-GMC
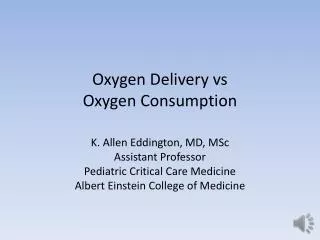
Aged 80 years in 1994Aged 80 years in 2020 AGE DEPENDENCY RATIO Proportion of population aged 80 years (%)
Comorbid medical illness / cognitive disorders • Sensory loss • Financial worries • Retirement • Dependency • Dying and death • Bereavement
3 D’s • Depression • Dementia • Delirium (check the pee, poop etc) • 2 Extra D’s • Drugs • Delusional sx (Psychosis in the Elderly) • Overview and cases of • DEPRESSION • MANIA • ANXIETY • PSYCHOSIS • DELIRIUM • DEMENTIA “I want to die in my sleep like my grandfather, not like the people kicking and screaming in the backseat of his car.” Sue McKay Geriatric Psychiatrist
73 year old woman who presents with 2 month history of tearfulness, loss of energy, apathy, inability to get out of bed in the morning, and insomnia with early morning awakenings. She describes increasing anxiety, an inability to cope, forgetfulness, problems reading or even watching TV, a 30 lb weight loss and feels very constipated. • She expresses a concern that something is wrong with her stomach. Her lower back has also been bothering her more. • She lost her husband 8 months ago and one of her children a little over 1 year ago. • She has a remote history of resected breast cancer and a more recent history of thyroid cancer which was resected 3 years ago. She also has a history of atrial fibrillation. She has no past psychiatric history and has always been able to cope with difficulties until recently. • She is on coumadin and a beta blocker.
What is in your differential diagnosis? • What kind of investigations would you order? • Assuming you believe her to be depressed what would be your plan of treatment? • Is there a reason for suggesting one antidepressant over another? • Assuming she does not have any response to treatment after 3 weeks what would you do?
Psychological • Depressed mood • Loss of interest or pleasure • Feeling worthless or guilty • Problems thinking or concentrating • Suicidal ideas or plans • Vegetative • Change in appetite or weight • Change in sleep • Loss of energy • Psychomotor changes • Associated (non-DSM IV) • Anxiety (brooding, obsessive ruminations) or phobias • Irritability • Excessive worry about physical health • Pain • Tearfulness
Response • (50% reduction in HAMD or MADRS) • Remission • (2/12 completely free of sx) plus functional recovery • Relapse • (reoccurance before 2/12) • Recurrence • (reoccurance after 2/12)
Initiate treatment with SSRI, SNRI, NRI, other Partial or no response after 4-6 wks of tx at adequate dosages R/A Diagnosis. Optimize dose Inadequate response Augment 1st Lithium 2nd atypical antipsychotic 3rd Lamotrigine 4th Thyroid T3 Switch to new antidepressant from a different class Combine 2 antidepressants from different classes Consider ECT at any time particularly when Very severe depression Not eating or drinking Catatonia Psychosis Suicide Risk Med Intolerance / Pregnancy Consider psychotherapy at any point particularly with early childhood trauma
BIO: • SIMILAR EFFICACY • SSRI’s (~equal DBPC trials (70/40% D/P response), SNRI’s (?lower remission rates, faster response), SARI’s, NaSSA’s, TCA’s, MAOIs, RIMA’s, NDRI’s. COMPARE pooled [n-33 DBPC] remission rates [SSRI/SNRI/P= 35/41/24%; n=3355/3410/932] Nemeroff 2004 WJP. Comparison trials have higher response and remission rates. • ADEQUATE TRIALS • Adequate trial 4-6 weeks (look for some response @ 2 weeks as a predictor of success). Switching amongst the same class may also work. Effective (Response: 70% w 1st, 70% w 2nd, 90% overall). BUT 50% discontinue in first 3/12, <30% complete full course of tx. Watch for adherence. • SPECIAL POPULATIONS • Some evidence for > efficacy in severe depression with TCA’s (Clomipramine study group although HAMD favors sedative ADs over celexa). • Atypical features: Better efficacy with MAOI’s. Recurrent & FHx of BAD consider Li. • Psychotic features: ECT vs add AAP to antidepressant. • ECT (particularly psychotic depression 95% RR). • Consider especially if situation is urgent, not eating.drinking, taking medication, suicidal, medication intolerance
AUGMENTATION • Augmentation: Li (11 w TCA’s studies (n=135), RR 52%, ? w SSRI’s), T3 (w TCA’s), MPH, tryptophan, low dose atypical neuroleptics (Nemeroff JCP 2005). Consider also DA agonists-pramipexole (Aiken JCP 2007), strattera, pindolol, buspar, tryptophan, lamictal. Combos: Buproprion (2D6 inhibition), NaSSA’s (Carpenter 99, Debonnel 2000), SARI’s (watch for SS), SSRI w Des (Nelson 99, 2000). Caution with MAOIs and SSRIs. MAOI can be combined with a noradrenergic agent b/o COMT. STAR*D augmentation in TRD. See next slide. • MEDICALLY UNWELL • Comorbid medical conditions, consider stimulants, which are relatively safe and work faster. Methylphenidate, dextroamphetamine, and modafinil (less inc in BP, also helpful with narcolepsy). • NEW OPTIONS • Novel agents on the horizon: duloxetine (balanced dual 5HT/NA agent with affects on pain), agomelatine (agonist MT1/MT2 antagonist 5HT2C helps with sleep few ASEs), Ketamine, Selegiline transdermal system (STS), released this year in the US, reduced risk of dietary restrictions at lower doses compared with standard MAOIs.
Rates of recovery vary with duration of unremitted symptoms • Kindling • Decrease in precipitators • Number of episodes increases risk of reoccurence
Thase-Rush Criteria: • Stage 1: Failure of an adequate trial of 1 class of major antidepressant • Stage 2: Failure of adequate trials of 2 distinctly different classes of antidepressant • Stage 3: Stage 2 plus failure of a third class of antidepressant, including a tricyclic antidepressant (TCA) • Stage 4: Stage 3 plus failure of an adequate trial of a monoamine oxidase inhibitor (MAOI) • Stage 5: Stage 4 plus failure of an adequate course of electroconvulsive therapy (ECT) • Options • Switch antidepressants • Different or same class • Augmentation • Another antidepressant • Mood stabilizers: Li, Lamictal • Atypical antipsychotic • Dopaminergic agents • Stimulants • Psychotherapy • ECT • Experimental: TMS, VNS • See slide on reasons for tx resistance
Controversy exists still about whether depression in late life is assoc with poorer outcome • Post Hoc analysis of the Sequenced Treatment Alternatives to Relieve Depression (STAR*D). • Early onset age<55. Late onset age 55-75. (n=574) with non psychotic MDD with baseline HAMD>14. Citalopramx14 weeks. Outcome: 16 item Quick Inventory of Depressive Sx-self rated score. • Time to remission, remission rates did not differ between the groups. Am J Geriatr Psychiatry 2008 • (Next 2 slides for details….)
In the Elderly • Community studies • have shown that 25% of elderly persons report having depressive symptoms, but only 1% to 9% meet the criteria for major depression Lebowitz BD JAMA 1997. • Prevalence varies according to the population. • Higher prevalence rates are reported in the hospitalized elderly (36% to 46%), those who receive homecare 13.5% (Hybels Clinics in Ger Med 2003) and • those in long-term care facilities (10% to 22%) Teresi J. Soc Psychiatry Psychiatr Epidemiol 2001
More likely to have somatic complaints, anxious, melancholic and psychotic features. Therefore ECT often used and is effective. • Similar response rates (although may take longer to tx), high relapse rates. Only 10-20% are tx resistant. With aging, more frequent episodes and longer untreated episodes (duration to spontaneous remission is longer) or may change to chronic course. • May have comorbid cognitive impairments. Non-compliance and physical disability often lead to chronicity. • More often confronted by death, grief may be a complicating feature
Depression • Persistent mood state • Poor self esteem (from Mourning and Melancholia, Freud: introjected lost object w negative assoc feelings experienced as part of self) • Fxnal impairment beyond 2/12 • Suicidal thoughts with desire to die • Grief • Dysphoria, sadness comes in waves with marked fluctuation, often w triggers • No fxnal impairment > 2/12 • No psychomotor retardation, active suicidality, psychosis (although transient phen may occur) • Bowlby • Phases of Uncomplicated Grief (PSDR) • Acute despair/protest, denial (numbness, outbursts, anger) • Yearning / searching for deceased (restlessness, preoccupation w deceased) • Disorganization + despair (going through the motions, withdrawn, apathetic) • Reorganization (can think of loved one w joy/sadness • Grief in Children • Protest, Despair, Detachment • Kubler Ross • 1) Shock/denial, 2) anger, 3) bargaining, 4) depression, 5) acceptance
The following is true regarding depression • it is a treatable condition that with antidepressants has a remision rate of 30-40% and response rates of 67-90% • the neurotransmitters serotonin and noradrenaline are involved c) Psychotherapy is effective in severe depression d) an association between early life trauma, hippocampal atrophy and depression can be seen • it often presents with multi-system physical complaints • it is associated with coronary artery disease, stroke, diabetes, cancer, Parkinson’s, and MS. • ECT should be considered only when all other treatments have failed
Depression in old age: • Is more prevalent in women than men • Prevalence rates rise sharply with age • Is accompanied by a much lower suicide risk than in younger adults • Is unresponsive to treatment in half of cases. • Is often precipitated by a loss • Both b) and d) • Both a) and e)
Psychotic Depression: a) Is more frequent in elderly. b) Remits with antidepressants in 50% of cases c) Remits with antidepressants + antipsychotics in 75% of cases d) Responds and remits best with ECT e) Should prompt thorough search for symptoms of bipolar illness in pt and family members. f) All of the above except b) g) All of the above except b) and c)
Which of the following are frequent “reason for consultation” by elderly who have their first depressive episode: MCQs a) “Nerves” b) Excessive fatigue c) Hypersomnia (sleeping too much) d) Digestive problems e) Fear of Alzheimer’s disease
MCQs a) Active suicidal ideation b) Prominent psychotic symptoms c) Crying spells when she thinks of her deceased husband. d) Being less active socially e) Being unable to attend to her usual daily activities 3 months after the death of her husband
76 year old who presents with decreased sleep, increased activity, mood lability with both tearful episodes and euphoria, 20 lb weight loss, irritability, circumstantiality, ruminations about perceived injustices in the past, and a concern over a conspiracy that involves his family physician, friends and neighbours. • He was started on Prednisone for a skin condition two weeks preceding these changes. • Because he is convinced he is invincible and his behavior started to include reckless and dangerous activities he was admitted to hospital.
MANIC/HYPOMANIC EPISODE E with 3/7 or I with 4/7 for 1 week Hypomania same but for 4 days no psychosis, no severe impairment, no hospitalization Mixed episode criteria met simultaneously for MDE and ME nearly every for at least 1 week. G grandiosity I increased goal directed activity D decreased judgment D distractibility I irritability N need for sleep decreased E euphoria S speedy thoughts S speedy talk • BAD specifiers • Type I [Mania] • Type II [No hx of mania but episodes of hypomania] • Most recent episode • Rapid cyclers (>4 mood episodes per yr) • DDx: ME • GMC • Substance induced • MDE w irritable mood • Mixed episode • ADHD • Psychosis
B- Determine phase of illness MDE,M, ME,E • Mania: start or optimize monotherapy: • Li or VPA, consider augment w AP (particularly w psychotic features), benzo. If no response combine other (Li or VPA). Mixed or dysphoric (?comorbid subs abuse): VPA may be better. Usually depressive sx are residually present. Another option is OLZP (2 large RCT’s- Tohen 10 mg, AJP 1999, Tohen 15 mg AGP 2000) w comparable efficacy to Li, VPA, Haldol. > than VPA in comparison trial. Risp and Zip studied in PCT as add ons to Li or VPA w efficacy comparable to Haldol>PCB. • Depression: do not start an antidepressant without a mood stabilizer. Lithium monotherapy should be considered. • Lithium (8 PCT’s 79% response) or Lamotrigine (Calabrese JCP 1999: MADRS 200>50mg/d>PCB , n=195 BAD-I). AD monotherapy not recommended b/o switch +/- rapid cycling. Buproprion (2 controlled add on studies 1st = efficacy to Des but less manic switch, RIMA (comparable to IMI w less ASE), Paxil 3 double blind add on studies, 1st good response=add on of other (ie. of either VPA or Li), no difference if Li > 0.8, sim to Effexor but less manic switch. AAP improve depression subscales in tx of Mania and extension trials.
B- Determine phase of illness DE,M, ME, • Maintenance: Only Lithium supported by RPCT’s although some design limitations. One negative PC comparison trial w VPA (Bowden AGP 2000). VPA studied in comparison w Li but no PC. • Specific Meds: Lithium (Cade’s disease: for mania, depression, relapse prevention 5 PCTs >25y ago), Epival (rapid cycling, dysphoric, mixed episode, efficacy in mania but prophylaxis data lacking). Alternatively monotherapy w AAP. Lamotrigine appears helpful w depression (Calabrese JCP 1999) , rapid cycling (BAD-II) (Calabrese JCP 2000), but not mania). Topimax (no PCT, studied as add on cf buproprion: McIntyre Acta Neuropsychiatr 2000), GABApentin. OLZP and more atypical studies pending. Also consider Clozapine in tx resistant cases. • ECT for tx resistant acute mania or depression (particularly w psychotic features).
P- Establish therapeutic alliance, individual psychoed intervention, interpersonal and social rhythm therapy [helps correct sleep] which decreases relapse risk. Prelim studies suggest that CBT may help reduce depressive sx, improve longer term outcomes and adherence. Supportive therapy may also be helpful (social skills help, coping skills, problem solving. • S- Involve family. Family interventions and focused therapy can helping to accept illness, identifying precipitating stressors inside and outside of family, examining family interactions that produce stress in the pt, developing management plan: these all lead to reduced relapse rates. Housing, work/vocational support. Collaborate to address comorbidity. Case management, ACT, rehab, should be considered.
More secondary mania (less often +FHx). • More mixed/dysphoric features with irritability but lithium response rate similar in young and old. Longer acute episodes. Increased frequency, higher prevalence of neurological abnormalities • Less hyperactivity, grandiosity, less euphoria, flight of ideas although may have disorganization and circumstantiality as well as delusions. • Secondary Causes of Mania in Elderly • Extrapyramidal disease, subcortical dementias, HIV, CNS infections, tumors, Demyelinating disease, Temporal lobe epilepsy, Systemic illness, Hyperthyroidism, uremia, pellagra • Drugs: steroids, L-dopa, amphetamines, cocaine, cyclobenzaprine (Flexeril), yohimbine (Aphrodyne), clarithromycin (Biaxin) • C-L service: steroids, HIV, TLE • Rundell JR, Wise MG (1989), J Neuropsychiatry ClinNeurosci
Which of the following is true of Bipolar disorder • Depression is the most debilitating and treatment resistant phase of the illness • Lithium has the best evidence for the treatment of depression, mania, suicide risk reduction and maintenance • Their exists double blind placebo controlled evidence for the use of Epival in depression and for the maintenance phase of the illness • Lamotrigine has been shown to be an effective antimanic agent • There is evidence for the use of atypical antipsychotics in mania • Olanzapine and Seroquel have been studied in a placebo controlled fashion for the depressive phase. • Clozapine can be used for treatment refractory cases
MCQs Compared to younger manic patients, elderly manic patients seem to have: • Less hyperactivity • More mixed (depressive/manic) clinical presentations • More disorganised speech with flight of ideas. • More irritability and less euphoria • Less paranoid delusions
Anxiety Disorder Mood Disorder • Fear • Apprehension • Panic attacks • Chronic pain • GI complaints • Excessive worry • Agitation • Difficulty concentrating • Sleep disturbances • Depressed / irritable mood • Anhedonia • Euphoria • Weight gain/loss • Loss of interest • Hypervigilance • Agoraphobia • Compulsive rituals APA 1994; Keller MB 1995; Clayton PJ et al 1991; Coplan JD, Gorman JM 1990
As many as 90% of depressed patients suffer from anxiety symptoms1-3 • More severe illness at baseline • More psychosocial impairment • Greater likelihood of chronic illness • Poorer, slower response to treatment • Greater likelihood of committing suicide What is primary? 1. Richou H. et al. Human Psychopharmacol 1995; 10:263-71 2. Coplan JD et al. J Clin Psych 190; 51(Suppl 10):9-13 3. Kasper S. et al. Primary Care Psych 1997; 3:7-16
Secondary anxiety disorders more common in elderly • Primary anxiety disorders, like personality disorders, generally do not have an onset in the elderly • High comorbidity with depression • Overally less common in the elderly. • Phobias and GAD are the most common. Panic disorder is relatively rare, less than the 1-3% described in younger populations (Flint AJP 1994). • Caution with anxiolytics • can cause paradoxical disinhibition • Diphenylhydramine (Benadryl), Dimenhydrinate (Gravol), Chlorpromazine, Amitriptyline, chloral hydrate and barbiturates are not good anxiolytics for older patients due to their side effects • Elderly are more sensitive to benzodiazepines. Associated with an increased risk for falls and MVAs
Cognition • Amnesia specially in alcoholics with benzos • Memory and visuospatial impairment • Psychomotor • Accentuate postural sway and coordination • Increase risk for MVAs and falls • Paradoxical dysinhibition • Respiratory Depression • avoid benzos in sleep apnea • Sleep • Decreased sleep latency but also decreased stage 3 and 4 sleep with Benzos
The following is true of anxiety disorders in old age a) It is more often secondary to another axis 1 condition like depression or medical condition b) Anxiolytics can worsen not only anxiety but can cause sleep disruption, falls, and MVAs. c) Benzodiazepines are safe in the elderly • Benadryl, Gravol, Chlorpromazine, Amitriptyline and other anticholinergic medications can be dangerous in the elderly because of delirium and associated other receptor effects (orthostatic hypotension) • Primary anxiety disorders and personality disorders, including dependent personality disorder, do not begin in old age
The following is true of anxiety disorders in old age a) It is more often secondary to another axis 1 condition like depression or medical condition b) Anxiolytics can worsen not only anxiety but can cause sleep disruption, falls, and MVAs. c) Benzodiazepines are safe in the elderly • Benadryl, Gravol, Chlorpromazine, Amitriptyline and other anticholinergic medications can be dangerous in the elderly because of delirium and associated other receptor effects (orthostatic hypotension) • Primary anxiety disorders and personality disorders, including dependent personality disorder, do not begin in old age
MCQs a) Prevalence rates increase with ageing. b) Phobias are the most common anxiety disorder c) Overall prevalence rates for all anxiety disorders in old age is around 10% d) Panic disorder affects approx. 5% of elderly.
85 year old woman who lives alone, never married and has no children. She is hard of hearing and visually impaired. • She has become increasingly seclusive and withdrawn. Her hydro and water stopped being paid and was cut off. • A nephew who was concerned called the CCAC to ask if someone could check in on her and help her at home. She refused to allow anyone in and talked about a how people were trying to break into her house and kill her. She was convinced the mail man was delivering messages from the devil.
In the Elderly • PRIMARY PSYCHOTIC DISORDERS • Schizophrenia • Late onset 25% • Early onset grown old 75% • Delusional Disorder • 0.03% but 1-2% of hospital admissions • Paraphrenia • MOOD DISORDERS • Depression • (33% of severe subtype cf 15% mild to moderate) • Mania • COGNITIVE DISORDERS • Dementia • (~50% have psychotic symptoms) • Delirium • Substance-GMC ALL • Psychosis • Substance - GMC • Mood D/O (MDD or BAD) • SCZ, SCZ-A • BPE • Dissociative D/O • Delusional disorder • Delirium • Personality disorders
PRIMARY • Schizophrenia • Bizarre delusions • Absence of memory problems, disorientation • Schizoaffective • Delusional disorder • MOOD • Depression • Mood, somatic (often bowel), anxious sx, real or perceived losses, phx/FHx of depression • Mania • More mixed states in the elderly, dysphoria, less grandiosity • COGNITIVE • Delirium • Reversed sleep cycle, marked variation, hallucinations, recent drugs, ETOH, intox/withdrawal • Dementia • By history • Cortical / subcortical syndromes • Neuropsych
Which of the following are not true of psychotic disorders in late life? • Most paranoid disorders of old age are due to schizophrenia [Jeste 2000]. • More women develop late onset schizophrenia [Jeste 2000]. • With ageing, schizophrenia tends to give less severe positive symptoms [Jeste 2000]. • Patients with schizophrenia live 10-30 years less on average [Harris BJP 98, Colton Prev Chron Dis 2006, Hennekens Am Heart J 2005] • There is some evidence that the elderly are less likely to experience the same metabolic side effects as younger patients do with atypical antipsychotics [Herrmann Drug Safety 2006]
68 year old woman who you, as her family physician have followed over many years, presents with increasing confusion, gait instability, falls, and incontinence. The change appears abrupt. She is now sleeping much of the day and is up at night. • She is on several medications including beta blockers, diuretics and Mobicox for arthritis. She continues to have some brandy after supper. When she last came to the clinic you were away and a locum prescribed some clonazepam to help her sleep better and relieve some of her anxiety. • She is admitted to the hospital under your care. • What is in your differential diagnosis? • What tests would you order?
A urine C&S and CT head were normal. • Routine blood work was also normal. • She is now extremely agitated at night. Falling frequently and is distressed with the belief that people are trying to kill her and she has to escape out of this prison. The nurses on the floor are requesting sedation or restraints for safety. • What are your next steps and why?
Meagher (1996), BJP • Hypo: dec Ach in nucleus basilis & RAS, associated with CVA, metabolic disorders, late sepsis, aspiration, pulmonary embolism, decubitus ulcers and other complications related to immobility. Characterized by: Unawareness, inattention, decreased alertness, sparse or slow speech, lethargy, decreased motor activity, staring, apathy. Liptzin (1992) BJP • Hyper: withdrawal states, acute infection, mediated by LC-NA. • Etiology: Hyper and hypactive delirium • Ach in RAS (dorsal tegmental pathway). • Risk factors • Medical illness, sensory impairment, hx of delirium, ETOH, pre-existing brain damage (eg. Dementia), malnutrition • Disturbance of 4Cs • C Consciousness (focus, sustain or shift attention) • C Cognition (memory, disorientation, language) or perceptual disturbance • C Course • C Consequence of GMC • Delirium in the elderly patient is associated with increased mortality, longer hospital stays, and increased risk of institutional placement. • Subcategories: • due to GMC, substance intoxication/withdrawal, multiple etiologies • Prevalence: 10-15% of those hospitalized. Under recognized. in those >65 higher (10-40%). • Independent risk factor for mortality 40% @ one yr. Lab features: EEG generalized slowing