Download
1 / 24
240 likes | 506 Vues
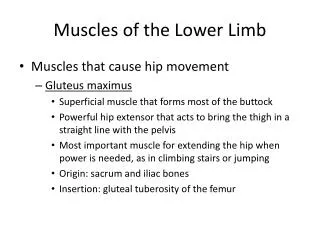
Muscles that Abduct the Femur at the Acetabulofemoral (Hip) Joint. Primary Hip Abductors. Gluteus Medius Gluteus Minimus Tensor Fascia Latae. Primary Hip Abductors. The hip abductors prevent adduction of the hip The hip abductors prevent the pelvis from falling when standing on the same leg

E N D
Muscles that Abduct the Femur at the Acetabulofemoral (Hip) Joint
Primary Hip Abductors • Gluteus Medius • Gluteus Minimus • Tensor Fascia Latae
Primary Hip Abductors • The hip abductors prevent adduction of the hip • The hip abductors prevent the pelvis from falling when standing on the same leg • If the hip abductors were too weak they would allow the opposite side of the pelvis to drop
Gluteus Medius Origin • External surface of Ilium between anterior and posterior gluteal line Insertion • Greater Trochanter of Femur Action • Abduction of Femur (entire muscle) (frontal plane and transverse plane) • Medially/Internal Rotation of Femur (anterior fibers) • Lateral Rotation of Femur (posterior fibers) • Depression of Pelvis
Gluteus Medius • Depression of the pelvis is its most important action. • When one foot is lifted off the floor (walking and running) The gluteus medius contracts to stabilize the pelvis and prevent sagging on the unsupported limb. • When the left muscles are contracted, the right side is prevented from sagging as the right limb is raised during walking.
Gluteus Medius • Stand and rock your weight back and forth from one foot to the other while palpating both gluteus muscles • The gluteus medius on the support side (the side that you are bearing your weight on) will be felt as it contracts
Gluteus Minimus Origin • External Surface of Ilium between anterior and inferior gluteal lines Insertion • Greater Trochanter of Femur Action • Abduction of Femur • Medial/Internal Rotation of Femur • Depression of Pelvis
Gluteus Minimus • Gluteus minimus is deep to gluteus medius • As with gluteus medius, pelvic depression is its most important action
Gluteus Medius and Minimus • Integrated Function: • Assists in eccentric deceleration of hip adduction • Assists in eccentric deceleration of hip lateral rotation • Assists in dynamic stabilization of the lumbo-pelvic hip complex
Tensor Fascia Latae The name tells us that this muscle “tenses” the fascia that lies over the muscles of the thigh Origin • Anterior Superior Iliac Spine and Anterior Part of Iliac Crest Insertion • Iliotibial Band which attaches to the Lateral Condyle of Tibia
Tensor Fascia Latae Action • Abduction of Femur • Medial Rotation of Femur • Flexion of Femur • Anterior Tilt of Pelvis • Depression of Pelvis
Tensor Fascia Latae • Integrated Function: • Assists in eccentric deceleration of hip adduction • Assists in eccentric deceleration of hip extension • Assists in eccentric deceleration of hip lateral rotation • Assists in dynamic stabilization of the lumbo-pelvic-hip complex and the tibio-femoral joint
Tensor Fascia Latae • There are two muscles that attach into the iliotibial band, the tensor fascia latae and gluteus maximus • Tensor Fascia Latae stabilizes the knee laterally. It prevents collapse of extended knee in ambulation.
Iliotibial Band Syndrome (ITBS) • The main problem occurs when the tensor fasciae latae muscle and iliotibial band become tight. • This causes the tendon to pull the knee joint out of alignment and rub against the outside of the knee, which results in inflammation and pain.
Iliotibial Band Syndrome (ITBS) • Is the most common cause of lateral knee pain among athletes • In the US: ITBS is the most common cause of lateral knee pain in runners with some studies citing an incidence as high as 12% of all running-related injuries • Develops as a result of inflammation of the bursa surrounding the iliotibial band. • Generally affects athletes who are involved in sports that require continuous running or repetitive knee flexion and extension such as long-distance running or cycling. • May be observed in athletes participating in volleyball, tennis, soccer, skiing, weight lifting, and aerobics.
Causation of ITBS Overload: • Exercising on hard surfaces, like concrete, or uneven ground • Beginning an exercise program after a long lay-off period • Increasing exercise intensity or duration too quickly • Exercising in worn out or ill fitting shoes • Excessive uphill or downhill running Biomechanical errors: • Leg length differences • Tight, stiff muscles in the leg • Muscle imbalances • Foot structure problems such as flat feet • Gait, or running style problems such as pronation
Treatment of ITBS Short Term: • Decrease mileage • Ice knee after activity. Massage. • Alternate running direction on a pitched surface • Lateral sole wedge (orthotics) to lessen pressure on the knee • Stretching glutes and TFL Muscles Long Term: • Stretching, especially before working out, to make the band more flexible and less susceptible to injury. • In extreme cases, surgery to relieve tightness in the band
Side Plank with Hip Abduction • Maintain neutral spine • Activate the core by drawing in • Start in a side plank position • Straighten the top leg into triple extension (at hip, knee, and ankle). • Perform side bridge and HOLD, then move top leg slowly into abduction and adduction. • Watch for external rotation in the top leg and for flexion of the hips… if noticed may need more stretching or more cueing
Standing Abductor Straight Leg Stretch • Benefits : • Increased function and ROM of the lateral hip • Preparation : • Stand as pictured with stretching leg crossed in behind. • Movement : • Laterally flex away from stretching leg until stretch is felt, hold for 20-30 seconds, repeat 2-3 times.
Supine Abductor Stretch Straight Leg with Rope • Benefits : • Increased function and ROM of the hip abductors • Preparation : • Position rope/band around the forefoot. • Movement : • Use rope to adduct leg until stretch is felt, hold for 20-30 seconds, relax and repeat 2-3 reps.
Assisted Supine Abductor Stretch Straight Leg • Benefits : • Increased function and ROM of the lateral hip musculature. • Movement : • Instruct person to actively adduct the leg as far as can be controlled, once at the endpoint, gently assist a few degrees further, hold for 20-30 sec seconds, relax, and repeat for 2-3 reps.
Abductor Rollup • Lay on your side with a NEUTRAL SPINE. • This means hips stacked, shoulders stacked, and something under the head to keep cervical neutral. • Maintaining neutral spine, and legs straight, EXTERNALLY ROTATE the entire top leg. • Generate ALL motion from the HIP allowing no compensation/movement anywhere else in the body. • Hold at end range briefly, return to starting position and repeat. • 1 set of 5-10 reps.