Download
1 / 27
290 likes | 573 Vues
Trauma Patients and Acute Respiratory Distress Syndrome. Definition. A syndrome of acute respiratory failure characterized by non-cardiac pulmonary edema and manifested by refractory hypoxemia caused by intrapulmonary shunt and diffusion barrier. Direct Injury.

E N D
Definition A syndrome of acute respiratory failure characterized by non-cardiac pulmonary edema and manifested by refractory hypoxemia caused by intrapulmonary shunt and diffusion barrier
Direct Injury • Chest trauma – pulmonary contusion • Near-drowning • Hypervolemia – pulmonary edema • Inhalation of toxic gases and vapors • Pulmonary embolism • Pneumonia (viral, bacterial or fungal)
Indirect Injury • Sepsis • Shock or prolonged hypotension • Multi-system trauma, especially multiple fractures • Burns • DIC • Acute pancreatitis • Head Injury • Abdominal trauma • Multiple blood transfusions
Pathophysiology • Onset of symptoms is usually 12 – 48 hours after time from acute injury • Has acute and chronic phases
Acute phase Acute lung injury Reduces normal perfusion to the lungs Causes platelet aggregation and stimulation of the inflammatory-immune system
Acute phase Release of mediators of the inflammatory process Mediators activate neutrophils, macrophages and other cells to release toxic substances that cause microvascular injury
Acute phase Acute and diffuse injury to endothelium and epithelium surface of lung occur Damage to pulmonary capillary membrane and increase in capillary permeability occurs
Acute phase Capillary leak allows proteins and fluids to spill into the interstitium and alveolar spaces Pulmonary lymphatic drainage capacity is overwhelmed and alveolar flooding occurs
Acute phase Pulmonary edema results and causes interference with oxygen diffusion and inactivation of surfactant Alveolar collapse and massive atelectasis occur and decrease functional residual capacity and lung compliance
Acute phase Profound hypoxemia related to extensive shunting (V/Q mismatch) Vasoconstrictive mediators cause increased pulmonary vasoconstriction and pulmonary hypertension
Chronic phase Type I pneumocytes are destroyed and replaced by type II pneumocytes which proliferate Interstitial space expands by edema fluid, fibers and proliferating cells Hyaline membranes are formed which increase the thickness of the alveolar-capillary membrane Pulmonary fibrosis may occur
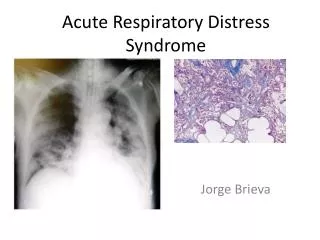
Clinical Presentation • Presence of a predisposing condition • Severe oxygenation defect – hypoxemia is the hallmark of ARDS • PaO2 < 60 mmHg on FiO2 > 50% • PaO2/FiO2 ratio < or = to 200 • CXR: diffuse bilateral parenchymal infiltrates • PAOP: < 18 mm Hg.
Clinical Presentation • Elevated PAP with normal PAOP (cardiac pulmonary edema causes elevated PAP and PAOP) • Pulmonary vascular resistance (PVR) is increased because of hypoxemic pulmonary vasoconstriction • ABG: Refractory hypoxemia
Pulmonary function studies • Lung volumes decreased: Tidal volume /vital capacity • Functional residual capacity decreased • Static and dynamic compliance decreased
Chest x-ray findings • Bilateral diffuse interstitial and alveolar infiltrates • Ground glass appearance • “White-out” due to massive atelectasis • Heart size is normal (unusual in cardiac pulmonary edema)
Ventilatory management • Modes: pressure control / inverse ratio ventilation or high-frequency jet ventilation may be used • Tidal volume: limitation of peak inspiratory pressure and reduction of regional lung overdistension by the use of low tidal volumes with permissive hypercapnia.
Ventilatory management • “Baby-lung” treatment: TV should be 4-8 ml/kg. - excessive volume forced into a small aerated lung can cause volutrauma • PaCO2 is allowed to gradually increase as minute ventilation is reduced – bicarbonate may be used in pH is less than 7.15 • Hypercapnia contraindicated with concurrent head injury
Ventilator management CPAP or PEEP • Decreases surface tension: keeps alveoli open • Aids in reopening collapsed alveoli • Reduces intrapulmonary shunt and increases functional residual volume • Obtain higher PaO2 with same or lower FIO2 • Usual level 5-15 cm H2O – may be higher
Ventilator management • FIO2 should be maintained as low as possible to prevent oxygen toxicity • Need nitrogen to keep alveoli inflated • CPAP may be administered via mask prior to intubation • Patients very PEEP dependent and will quickly desaturate when temporarily discontinued • Utilize transport ventilator when moving patient • May require sedation and/or paralysis to maintain PEEP
Intraalveolar fluid • CPAP or PEEP increases intraalveolar pressure – prevents further fluid sequestration into the alveoli • Diuretics may be considered - maintain PAOP at ~ 12 mmHg • Colloids leak across the alveolar-capillary membrane as readily as crystalloids
Hemodynamics • Inotropes as indicated by cardiac index/output • Dobutamine is usually the first choice • Best PEEP = in PaO2 and SaO2 but does not cardiac output
Other therapies Nitric oxide: Synthesized by vascular endothelium and acts as a natural localvasodilator when inhaled – it dilates vessels only to ventilated areas and acts as a potent bronchdilator More effective when used during early stages
Other therapies • Corticosteriods: May be helpful during the fibroprofilerative phase • Nutritional support: To prevent respiratory muscle atrophy and translocation of bacteria from GI tract
Complications • Nosocomial pneumonia • Sepsis • Shock • Multiple organ dysfunction syndrome (MODS) • DIC • Airway trauma • Dysrhythmias • Pulmonary embolism • Pulmonary fibrosis • Barotrauma • GI hemorrhage • Renal failure
ARDS vs. Pulmonary Contusion • Pulmonary contusion is usually localized and occurs near the site of external trauma • ARDS causes diffuse bilateral changes • CXR with contusions show increased density reflecting intraalveolar hemorrhage