Radioimmunoassay and Insulin Determination
Radioimmunoassay and Insulin Determination. Radioimmunoassay. R adio i mmuno a ssay ( RIA ) is a very sensitive in vitro assay technique used to measure concentrations of antigens (for example, hormone levels in the blood) by use of antibodies.

Radioimmunoassay and Insulin Determination
E N D
Presentation Transcript
Radioimmunoassay • Radioimmunoassay (RIA) is a very sensitive in vitro assay technique used to measure concentrations of antigens (for example, hormone levels in the blood) by use of antibodies. • RIA technique is extremely sensitive and extremely specific, requiring specialized equipment.
History • The technique was introduced in 1960 by Berson and Yalow as an assay for the concentration of insulin in plasma. • It represented the first time that hormone levels in the blood could be detected by an in vitro assay. • The technique of radioimmunoassay has revolutionized research and clinical practice in many areas, e.g., • Blood banking • Diagnosis of allergies • Endocrinology
Principle • The technique is based on the ability of an unlabelled form of the substance to inhibit competitively the binding of a radioactively labelled substance by specific antibodies. I125 labeled antigen Ag in serum Ab for the Ag
It is based on a principle of serial dilutions. One starts with a combination of radioactively labelled antigen (corresponding to the hormone to be measured) and antibody to that hormone. • Then, a specific quantity of unlabeled, or cold antigen is added to the mixture. The unlabeled antigen competes with the radioactive antigen for binding to the antibody and displaces a proportional amount of it. The unbound antigen is separated away (by centrifugation, for example) and the amount of radioactivity remaining is measured.
This process is continually repeated, using progressively greater concentrations of unlabeled antigen, and a line graph demonstrating the relationship between concentration of the unlabeled antigen and the radioactivity remaining is constructed. • This process creates a standard binding curve. The competitive binding process is then repeated using the biological sample to be tested and by comparison the radioactivity resulting with the standard binding curve, one can deduce the concentration of the hormone in the sample of interest.
Method • To perform a radioimmunoassay, a known quantity of an antigen is made radioactive, frequently by labelling it with gamma-radioactive isotopes of iodine attached to tyrosine (hot). • Both 125I or 131I emit gamma radiation that requires special counting equipment. • This radiolabelled antigen is then mixed with a known amount of antibody for that antigen, and as a result, the two specifically bind to one another. • Then, a sample of serum from a patient containing an unknown quantity of that same antigen is added. • This causes the unlabeled (or "cold") antigen from the serum to compete with the radiolabelled antigen ("hot") for antibody binding sites.
As the concentration of "cold" antigen is increased, more of it binds to the antibody, displacing the radiolabelled variant, and reducing the ratio of antibody-bound radiolabelled antigen to free radiolabelled antigen. • The bound antigens are then separated from the unbound ones, and the radioactivity of the free antigen remaining in the supernatant is measured using a gamma counter. Using known standards, a binding curve can then be generated which allows the amount of antigen in the patient's serum to be derived.
Requirements for the development of RIA • Pure antigen : for standards (μg) • Tracer : self-made or commercial. • Specific, high-affinity antibody : self-made or commercial. • A method to separate bound and free antigen. • (Optional) : A system to extract the antigen from the sample.
Advantages Disadvantages • The main disAdvantages to radioimmunoassay are the expense and hazards if preparing and handling the radioactive antigen (hypothyroidisim) • Expensive equipment (gamma or beta Counter) • Radioimmunoassay is widely-used because of its great sensitivity. Using antibodies of high affinity, it is possible to detect a few pictograms (10−12 g) of antigen in the tube. • The greater the specificity of the antiserum, the greater the specificity of the assay
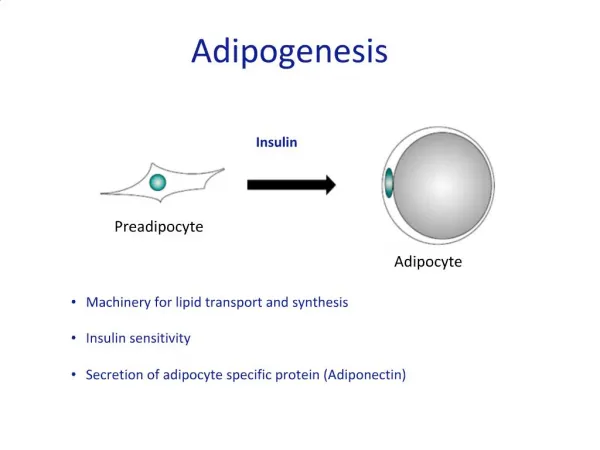
Insulin • Human insulin is a peptide produced in the beta cells of the pancreas and is responsible for the metabolism and storage of carbohydrates. • As a result of biofeedback the insulin levels increase with intake of sugars and decline when sugar content is low for absorption. • In the diabetic population the mechanism of insulin production is impaired because of genetic predispositions type1, or because of lifestyle and/ or hereditary factors type2. • in such cases either the insulin production has to be boosted by medication or it has to be supplemented of insulin can help in dose selection the patient has to be subjected to.
C-peptide • C-peptide is the abbreviation for connecting peptide; it is a 31-amminoacid peptide. • C-peptide of insulin is the C-terminal cleavage product produced during processing of the insulin pro-hormone to the mature insulin molecule. • Proinsulin is cleaved when it is released from the pancreas into the blood - one C peptide for each insulin molecule. • C-Peptide is devoid of any biological activity but appears to be necessary to maintain the structural integrity of Insulin. • The source of the insulin may be identified by simultaneous measurements of C- peptide: endogenous hyperinsulinism is accompanied by a raised c-peptide whereas exogenous insulins don’t contain c- peptide.
If a person is injecting insulin, measuring C-peptide is the only way doctors can determine whether they are also making insulin on their own; since lab tests do not distinguish between injected insulin and homemade.Some doctors prefer to measure C-peptide even in people not injecting insulin because of its longer life in the bloodstream which means you won't see as much fluctuation from moment to moment in C-peptide levels as you may find with insulin levels. • The C-Peptide test does not indicate whether the beta islet cells of the pancreas are working or not, nor whether there are in fact beta cells present. C-Peptide is not a test for insulin production, but a test for insulin released from the pancreas.
Functions of Insulin • Insulin helps muscle, fat, and liver cells absorb glucose from the bloodstream, lowering blood glucose levels. • Insulin stimulates the liver and muscle tissue to store excess glucose. The stored form of glucose is called glycogen. • Insulin also lowers blood glucose levels by reducing glucose production in the liver(gluconeogenesis) • It also inhibits gylcogenolysis and ketogenesis.
Insulin released after meal in response to a rise in plasma glucose. • Fasting suppresses insulin release to very low levels. • Insulin measurements are most useful when performed in the fasting state. For the investigation of hypoglycemia it is essential that glucose is measured simultaneously. • The diagnosis of diabetes is usually made upon the basis of history and blood glucose concentration in either the fasting state or after a glucose load and NOT upon the basis of plasma insulin concentration.
Clinical uses • Identification of the cause of hypoglycemia • Insulin is measured of the investigation of unexplained hypoglycemia, which usually occurs in infants or young children but may also occur in adults. • In normal person with normal insulin sensitivity, plasma insulin should be totally suppressed in the presence of hypoglycemia. • If this is not observed, it suggests that insulin is responsible for the hypoglycemia • Localization of an insulinoma.
Insulin resistance • Insulin resistance is a condition in which the body produces insulin but does not use it effectively. When people have insulin resistance, glucose builds up in the blood instead of being absorbed by the cells, leading to type 2 diabetes or prediabetes • Insulin resistance is present in many overweight or obese people, in whom insulin may be raised even during fasting. • Hyperinsulinism in the presence of normal or raised plasma glucose indicates insulin resistance and is a common finding in overweight people with or without type 2 diabetes. • Insulin resistance is best measurement by a using a complex euglycemic clamp technique requiring multiple measurements of both insulin and glucose.
High value of insulin • Hyperinsulinism causing hypoglycemia may be seen in: • Infants of diabetic mothers • persistent hyperinsulinemia • hypoglycemia of infancy. • Sulphonylurea(oral antidiabetic2 drug) or insulin overdose • Insulinoma • The presence of autoantibodies to insulin or insulin receptor.
Investigation • In hyperinsulinemia hypoglycemia, further investigations may include measurements of serum c-peptide and serum or urine sulphonyureas, and pancreatic imaging. • Further investigation of insulin resistance is generally not required. • It is elevated in patient with an insulinoma and in those with excessive growth hormones secretion gigantism in children, acromegaly in adult. • Quantitation of plasma insulin is of no value in diagnosis of diabetes mellitus.
Low value of insulin • Low or undetectable insulin is an expected finding in the presence hypoglycemia or in the fasting state unless the individual is insulin resistance. • Type 1 diabetes and advanced type 2 diabetes are characterized by insulin deficiency leading to hyperglycemia. However, insulin measurement is not required to make these diagnosis.
Analytical issues • An insulin value alone is not of diagnostic value and should only be used in conjunction with other clinical manifestations and diagnostic procedures. Collection sample: • EDTA, Heparin sample • Serum • For accurate comparison to established normal values, a fasting morning serum sample should be obtained. • Samples may be refrigerated at 2-8c for a maximum period of five days. If the specimens cant be assayed within this time, the sample may be stored at temperature of -20C for up to 30 days.
MID TERM EXAM الثلاثاء 14/3/2017 الساعة 11:00 Labs 1(Introduction)-5(ELISA P2)