Download

1 / 102
1.02k likes | 1.24k Vues
TRI : An Emerging Mini-invasive PCI New Model from for the LM Bifurcation Lesion. Yuejin Yang MD, PhD, FACC Cardiovascular Institute and Fu- Wai Hopital, CAMS & PUMC. The 25 th Tian Jin Cardiovascular Circulation (TJCC ) 2011-5-22, T J, China. Contents. Why TRI ?

E N D
TRI : An Emerging Mini-invasive PCI New Model from for the LM Bifurcation Lesion Yuejin Yang MD, PhD, FACC Cardiovascular Institute and Fu-Wai Hopital, CAMS & PUMC • The 25th Tian Jin Cardiovascular Circulation (TJCC ) 2011-5-22, T J, China
Contents • Why TRI ? • TRI for complex lesions (feasible) ? • TRI for LM bifurcation (feasible) ? • Evolution of LM PCI • Strategic determinations • Technical considerations • Fu-Wai Experience • Warning for LM PCI • Conclusions
The Shortcomings of TFI • Forceful lying on bed: • undurable for patients • high risk of death for induced DVT+PE! • Complications at puncture site: • bleeding and hemotoma • also high risk of death due to post peritoneal bleeding! • Occlude device: • cost more
The Advantages of TRI • Free mobile post procedure : • unpainful and acceptable for patients • no risk of death induced by DVT+PE! • Less puncture site complications • no big hamotoma and • less risk of hemorhegic death! • Much less care work needed • Save human resources • No occlude device and short hos. stay: • cost less
The Differences Between TRI vs TFI • Access site: radial vs femoral A • Artery size : smaller vs bigger • Guiding size: 6Fr and under vs 6Fr and beyond • Major differences before guiding engagement, • Almost the same after guiding in place
Feasible Technically • The majority of TFI is routinely performed with 6Fr guiding. • The size of radial artery in the majority of Chinese adults also fits with 6Fr guiding. • TRI is actually as same as TFI with 6Fr guiding. • Routine TRI is as possible as TFI in daily practice with 6Fr guiding.
Numbers of PCI @ Fu Wai Each Year 80.22% in 2007
6000 5148 4778 5000 4326 3884 3840 PCI 4000 3283 2823 3000 TRI 2034 2000 1000 0 2005 2006 2007 2008 Numbers and Rates of TRI at Fu-Wai Hosptal in 2008 TRI account for 84%(4326/5148)
2011 PCI at FuWai CV Hosptal • PCI number: 8050 cases • Mortality rate: 0.05% ( 万分之五) • TRI:89.8%(90%) • 2011?Should be more! • In Mar:>1000 cases performed • Expected to reach 10000 cases in 2001 !
Key Skills for Successful TRI • Accurate radial A puncturing for successful cannulation • Gentle catheter forwarding and manipulating to avoid initiating radial A spasm • Unique guiding catheter manipulating for coronary ostium engaging. • Special guiding catheter choosing to get enough backup support
Principles For Guiding Catheter Selection in TRI • RCA :6F-JR4(80%). Amplatz L1 or XB-RCA (20%) • LAD :6F-JFL. EBU-3.5、XB-3.5、Amplatz L1 (>80%) and JL3.5 (20%) • LCX and CTO, long diffuse ,bifurcation, tortuous and angutating lesions (100%) :6F -JFL. EBU-3.5 、XB-3.5、Amplatz L1 • Kissing and crushing technique :6F-Luncher (larger lumen, ID0.071”)guiding catheter
The Dominances in TRI Techniques • Not only simple lesions • But also complex lesions & cases
New Technology Currently Used for Complex Lesions • For CTO: final stronghold antigrade approach retrograde approach • For LM: high risk one-stent techniques two-stent • For bifurcation: complicated One stent technique Two stent technique DK crush Cullotte SKS Provisional T TAP
New Technology for Complex Lesions in TRI • For CTO: anti-grade approach retro-grade approach? • For LM: one-stent technique two-stent techniques • For bifurcation: one-stent technique two-stent techniques step DK crush step DK inverse crush step cullotte step kissing stent Provisional T TAP
PCI for LM Bifurcation • High risk • Complicated
Evolution of LM PCI • PTCA:No, because of deadly acute closure ! • BMS: OK, no acute closure, acute/ subacute stent thrombosis also resolved, but high rate of restenosis. • DES: Yes, due to remarkable reduction in restenosis rate.
Dominances of LM PCI in DES Era • Remarkable reduction in restenosis rate (about 5-10%) • Remarkable reduction in revascularization rate (< 10%) • Much improved in stenting techniques one-stent two-stent • IVUS check • Dual antiplatelet therapy regimen
Clinical Evidence: Support of LM PCI • Clinical trial indicative of safty and efficacy DES vs BMS DES vs CABG • Randomized clinical tial DES vs CABG PES (Taxus) : SYNTAX SES( Sirolimus) : COMBAT • Guidelines: IIb indication
SYNTAX Trial Design 62 EU Sites 23 US Sites All Pts with de novo 3VD and/or LM disease (N=4,337) • Treatment preference (9.4%) • Referring MD or pts. refused informed consent (7.0%) • Inclusion/exclusion (4.7%) • Withdrew before consent (4.3%) • Other (1.8%) • Medical treatment (1.2%) 71% enrolled (N=3,075) + Heart Team (surgeon & interventionalist) Total enrollment N=3075 Amenable for both treatment options Amenable for only one treatment approach Stratification: LM and Diabetes DM 28.2% NonDM 71.8% Stratification: LM and Diabetes DM 28.5% Non DM 71.5% Randomized Arms N=1800 Two Registry Arms N=1275 Randomized Arms n=1800 Two Registry Arms PCI N=198 PCI all captured w/ follow up CABG N=1077 CABG n=1077 CABG 2500 750 w/ f/u CABG n=897 TAXUS n=903 PCI n=198 TAXUS* N=903 vs CABG N=897 no f/u n=428 5yr f/u n=649 vs LM 33.7% 3VD 66.3% LM 34.6% 3VD 65.4%
Adverse Events to 12 Months CVA (Stroke) All Death Myocardial Infarction Revascularization TAXUS* (N=903) CABG (N=897) ITT population Event Rate ± 1.5 SE, *Fisher exact test
Symptomatic Graft Occlusion & Stent Thrombosis to 12 Months TAXUS(N=903) CABG(N=897) P=0.89 Patients (%) 3.4 3.3 n=27 n=28 CABG TAXUS ITT population
Death/CVA/MI to 12 Months TAXUS(N=903) CABG(N=897) 20 10 Cumulative Event Rate (%) 0 0 6 12 Months Since Allocation P=0.98* 7.7% 7.6% Event rate ± 1.5 SE. *Fisher exact test ITT population
MACCE† to 12 Months TAXUS(N=903) CABG(N=897) 20 10 Cumulative Event Rate (%) 0 0 6 12 Months Since Allocation P=0.002* 17.8% 12.1% Event rate ± 1.5 SE. *Fisher exact test †MACCE: Death, CVA, MI and Repeat Revascularization; ITT population
Patient Profiling Local Heart team (surgeon & interventional cardiologist) assessed each patient in regards to: Patient’s operative risk (EuroSCORE & Parsonnet score) Coronary lesion complexity (newly developed SYNTAX score) Goal: SYNTAX score to provide guidance on optimal revascularization strategies for patients with high-risk lesions SYNTAX score Number & location of lesions Dominance Left Main Calcification 3 Vessel Thrombus Total Occlusion Bifurcation Tortuosity EuroInterv 2005;1:219-227 • BARI classification of coronary segments • Leaman score, Circ 1981;63:285-299 • Lesions classification ACC/AHA , Circ 2001;103:3019-3041 • Bifurcation classification, CCI 2000;49:274-283 • CTO classification, J Am Coll Cardiol 1997;30:649-656 Sianos et al, EuroIntervention 2005;1:219-227 Valgimigli et al, Am J Cardiol 2007;99:1072-1081 Serruys et al, EuroIntervention 2007;3:450-459
MACCE to 12 months vs SYNTAX Score: Low scores (0-22) CABG(N=274) TAXUS(N=299) 30 20 Cumulative Event Rate (%) 10 0 0 6 12 Months Since Allocation P=0.71* 14.4% 13.5% RCT ITT pts; site-reported data Event Rate ± 1.5 SE; *chi square test; raw SYNTAX score for illustrative purposes only
MACCE to 12 months vs SYNTAX Score: Intermediate scores (23-32) CABG(N=300) TAXUS(N=310) 30 20 Cumulative Event Rate (%) 10 0 0 6 12 Months Since Allocation P=0.10* 16.6% 11.7% RCT ITT pts; site-reported data Event Rate ± 1.5 SE; *chi square test; raw SYNTAX score for illustrative purposes only
MACCE to 12 months vs SYNTAX Score: High scores (≥33) CABG(N=316) TAXUS(N=290) 30 20 Cumulative Event Rate (%) 10 0 0 6 12 Months Since Allocation P<0.001* 23.3% 10.7% RCT ITT pts; site-reported data Event Rate ± 1.5 SE; *chi square test; raw SYNTAX score for illustrative purposes only
LM PCI Strategic Determinations • PCI vs CABG selection • PCI itself strategies • One-stent • Two-stent • Crush or step crush • Cullotte • T or provisional T • Kissing or step kissing • Principal: safety first !!!
PCI vs CABG selection • Both technical mature and safety considered • Both technical mature and both safe: • CABG of choice, PCI second choice • PCI mature and safe : PCI • CABG mature and safe : CABG • PCI mature but high risk : No PCI • CABG mature but high risk : No CABG • Both technical premature : Neither CABG nor PCI • Both high risk : neither CABG nor PCI
LM PCI Itself Strategy • Procedural unrisk----safety first !!! • Procedural strategies---- feasibility • Acute outcome----in-hosp death & ST • Long-term outcome----MACE • Low risk (pure LM disease ) : PCI • High risk (LM+TVD) : No PCI • CABG recommended • Cardiac surgeon consulted
LM PCI: Technical Considerations • Experienced operators • Pre-determined strategy • Cardiac surgery stand-by and support • Emergency measures during procedure : device and drug • Pre-IABP (not stand-by): routine use for high risk patients • Routine IVUS check after procedure • Post-procedural monitoring (CCU)
LM PCI:Key Determinant Factors • Operators’ experience • Risk evaluation and comparison (PCI vs CABG) • LM function • LM lesion location and anatomy • Simple or complex LM with TVD • Durable dual antiplatelet therapy for at least one year • IVUS available • CCU available • Clinical and CAG follow-up
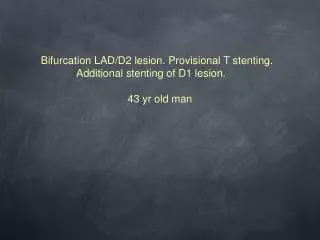
Shi JF F 64yrs 病案号:692169 09-8-24 • CABG for 3 months • LIMA 100%, • SVG-LCX 100% • LM bifurcation: 90% • Crush technique used • IVUS checked • Follow-up CAA(io-1-20) • SVG-RCA: patent
LM Reverse Crush Yang Peng M 79 Yrs No :709952, 2010-03-01 LM bifurcation both 90% LAD: CTO LCX: 90% RCA: unremarkable CABG indicated and suggested but declined by surgeon due to 慢淋 IABP used TRI+Reverse crush done IAPB rupture while withrawal and withdrawaled successfully
LM Body+Bfurcation Reverse Crush 李金平 M 82 Yrs 2010-03-03 Unique No:714400 LM body+bifurcation lesion:90% LAD: 80-90% CABG recommended but refused by Pts IABP TRI + reverse crush procedure Optimal results