Download
1 / 37
370 likes | 646 Vues
Gender-based Violence Female Genital Mutilation, Intimate Partner and Sexual Violence. Daisy Mafubelu Assistant Director-General World Health Organization Third African Conference on Sexual Health and Rights Abuja, Nigeria, 4-6 February 2008. WHO's Six-point Agenda.

E N D
Gender-based ViolenceFemale Genital Mutilation, Intimate Partner and Sexual Violence Daisy Mafubelu Assistant Director-General World Health Organization Third African Conference on Sexual Health and Rights Abuja, Nigeria, 4-6 February 2008
WHO's Six-point Agenda Commitment to have WHO be measured by the impact it will have on the health people of Africa and women • Addressing health development needs • Addressing health security needs • Strengthening health systems • Gathering, analysing and using evidence • Managing partnerships to achieve best results in countries • Ensuring that WHO performs well substantial level strategic level operational level
Violence Against Women and the Millennium Development Goals • Working towards achievement of MDGs will reduce violence against women • Preventing violence against women will contribute towards achievement of MDGs • WHO has a strategy to accelerate progress towards the attainment of international development goals and targets related to reproductive health. The core goal of the this strategy, was reaffirmed at the 2005 World Summit when Heads of State and Government committed to "achieving universal access to reproductive health by 2015, as set out at the ICPD, and integrating this goal in strategies to attain the internationally-agreed development goals, including the Millennium Development Goals (MDGs)". • This is the highest level of endorsement of the critical role that sexual and reproductive health plays in achieving the MDGs. The UN General Assembly noted the Secretary General's report with the new target to "achieve, by 2015, universal access to reproductive health", integrated within the revised MDG framework. The inter-agency and expert group (IAEG) on MDG indicators has now issued a revised MDG monitoring framework which integrates the new target and includes four indicators for monitoring progress: contraceptive prevalence rate, unmet need for family planning, adolescent birth rate and antenatal care attendance
Female Genital Mutilation 6 February Zero Tolerance Against Female Genital Mutilation
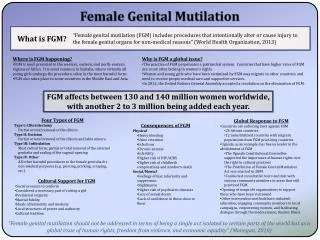
What is female genital mutilation (FGM)? FGM comprises all procedures involving partial or total removal of the external female genitalia or other injury to the female genital organs for non-medical reasons.
Prevalence of female genital mutilation • WHO estimates that between 100 and 140 million girls and women worldwide have been subjected to FGM Types I, II or III. • Estimates based on the most recent prevalence data indicate that, in Africa, 91.5 million girls and women aged 10 and above are currently living with the consequences of FGM. • An estimated 3 million girls in Africa are at risk of undergoing FGM every year.
Distribution of FGM in Africa and beyond UNICEF statistical overview 2005
Consequences of FGM • Severe pain is the most common immediate consequence of all forms of FGM. • The degree of pain and trauma is such that a woman or girl is often left in a state of medical shock after the operation. • Bleeding (Long-term anaemia also possible) • Damage to adjacent tissue • Urine retention • Keloid scars, abscesses and painful cysts. • In extreme cases: death due to severe and uncontrolled bleeding or to infection.
Consequences of FGM Continued FGM and obstetric outcomes: • Increased risk having cesarean section • Increased risk of having post partum hemorrhage, • Risk of perineal tear increased • Increased risk of perinatal death • Maternal mortality: no sufficient data
Medicalization of FGM • The position of WHO as regards the medicalization of FGM is consistent and unequivocal: “FGM of any form should not be practiced by health professionals in any setting-including hospitals or other health establishments”. • The World Medical Association and many national medical associations as well as the International Federation of Obstetrics and Gynecology (FIGO) have condemned FGM as unethical .
Role of Health Professionals in Eliminating FGM • Dr. Jon Snaedal, President of the WMA, said: "because of its serious detrimental impact on the physical and mental health of women and girls, female genital mutilation is a matter of deep concern to physicians. We are particularly worried to note the increasing practice of female genital mutilation by medical personnel. This is in contradiction with our code of ethics, as these practices violate the human rights of women and girls. The WMA is totally opposed to this medicalization of FGM". • He has called on all physicians and other health professionals to mobilise actively to stop these flagrant forms of violence against women.
WHO overall Strategy on FGM • To play an advocacy role by emphasizing the importance of action against harmful practices at international, regional and national levels. • To initiate and to coordinate the research and development being undertaken by • international agencies, nongovernmental organizations and national authorities. • To support national networks or organizations and groups involved in developing relevant policies, strategies and programmes. • To support the training of health professionals in the prevention of female genital mutilation and the management of its health consequences.
Elimination of female genital mutilation. An interagency statement • Signed by 10 UN agencies • Planned launch 27 February 2008 • Reinforce international commitment to eliminate the practice • Highlights human rights and legal dimensions of the problem • Series of actions that need to be taken by a variety of players such as Government, Parliamentarians, Professional Organizations, NGOs and FBOs, Community Leaders and Health Care Providers
Strategies for eliminating FGM • Long term, sustained and broad approach • Community engagement and ownership • Empowerment of women • Enactment and enforcement of laws • Culturally sensitive and effective approaches • Education and information measures • Develop material with people, discuss methods such as illustrations, photo, discussion groups, film etc. • Health system measures • Establish services for prevention, education, counselling and management of FGM by trained health staff • Implementation of medical ethical standards
Intimate Partner and Sexual Violence Sexual violence is: "any sexual act, attempt to obtain a sexual act, unwanted sexual comments or advances, or acts to traffic a person's sexuality, using coercion, threats of harm or physical force, by any person regardless of relationshipto the victim, in any setting, including but not limited to home and work" -WHO World Report on Violence and Health (2002)
Sexual violence takes many forms • Rape by strangers and within marriage or dating relationship • Systematic rape during armed conflict • Sexual abuse of children • Forced marriage or cohabitation (incl. of children) • Forced pregnancy • Forced abortion • Forced prostitution and trafficking of people for the purpose of sexual exploitation • Harmful traditional practices (FGM)
Findings from the WHO multi-country study on women’s health and domestic violence
Global study with interviews with 24 000 women in 10 countries Serbia and Montenegro Japan Thailand Bangladesh Ethiopia Samoa United Republic of Tanzania Peru Namibia Brazil Countries with one study site Countries with two study sites New Zealand
Objectives • Estimates of prevalence of violence against women • Associations between partner violence and health outcomes • Risk and protective factors for partner violence • Strategies used by women who experience partner violence (who do they talk to, where do they seek help, what response do they get)
Physical and sexual violence is extremely common in women’s lives
Domestic violence is prevalent but the level varies greatly among settings %
Types and patterns of violence vary between and within countries %
The younger a woman's age of first sex, the risk of a forced first sexual experience is higher % Note: Japan city, Serbia and Montenegro city and Thailand city are not represented due to low percentages reporting first sex before age 15 yrs.
Pregnancy is not necessarily a protected time He hit me in the belly and made me miscarry two babies - identical or fraternal twins, I don’t know. I went to the hospital with heavy bleeding and they cleaned me up Woman interviewed in Peru 28 15 12 12 11 10 10 8 8 7 6 4 4 3 1
Violence has negative pregnancy outcomes • late entry into prenatal care • increased smoking and substance use • vaginal and cervical infections • premature labor • miscarriages/abortions • bleeding during pregnancy • low birth weight
Violence impacts on women’s health and wellbeing I suffered a long time and swallowed my pain. That is why I am constantly visiting doctors and using medicines. No one should have to do this Women who have ever experienced violence by a partner have: Worse self-reported general health More symptoms of ill health such as pain, memory loss, dizziness in the past 4 weeks More signs of mental distress More suicidal thoughts and attempts More induced abortions and miscarriages
Partner violence increases risk of suicidal thoughts I don’t feel well and I just cry. There are times that I want to be dead. I even thought of killing myself or poisoning myself and my kids, because I think if I have suffered that much, how much would my kids suffer if I am no longer there…
Violent acts as a risk factor for ill health An association between recent ill health and lifetimeexperiences of violence suggest that the negative consequences of violence can persist long after the violence has ended
Many women internalize social norms justifying abuse My husband slaps me, has sex with me against my will and I have to conform. Before being interviewed I didn't really think about this. I thought this is only natural. This is the way a husband behaves Woman interviewed in Bangladesh
Violence is largely hidden One-fifth to two-thirds of women had never told anyone about their partner’s violence prior to the WHO interview If I protest I’ll be marked in the society and then my daughter wouldn’t be able to get married… If I voice my protest the community will blame me for not bearing it in silence. This helplessness is a torture in itself.
Violence is preventable • Violence against women represents a hidden burden on health systems • The variation in levels of violence across settings illustrate that violence is not inevitable
An integrated response is needed Prevention campaigns • Changing social norms that support and condone violence • Children and young people need to be educated in social skills needed to handle conflict and have healthy relationships • Schools need to be safe places Response to violence • Train doctors and nurses to identify women living with violence, and integrate into sexual and reproductive health programmes (e.g.family planning, antenatal care, post abortion care) • Create awareness at family and community level and overcome barriers to women seeking formal help