Download
1 / 27
270 likes | 592 Vues
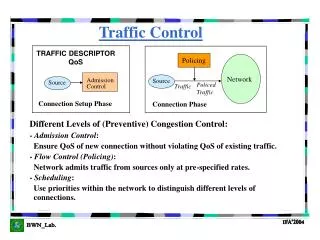
Traffic Control Strategy in SARS Outbreak Control. Muh-Yong Yen, Yu-sen E. Lin, Ih-Jen Su, Mei-Shang Ho, Kuang-Huan Tan, Chen-Hsen Lee Jen-Ai Municipal Hospital, Taipei City Veterans General Hospital, Kaohsiung. STOP SARS at the bedside. Life finds the way

E N D
Traffic Control Strategy in SARS Outbreak Control Muh-Yong Yen, Yu-sen E. Lin, Ih-Jen Su, Mei-Shang Ho, Kuang-Huan Tan, Chen-Hsen Lee Jen-Ai Municipal Hospital, Taipei City Veterans General Hospital, Kaohsiung
STOP SARS at the bedside Life finds the way SARS is looking for the niche/leak to jump into next victims (HCW)
Niche, leak • Waves niche reasons/solution • 1st wave 20-30 % mask & glove • 2nd wave 3-5 % PPE, NPIR • 3rd wave 1 – 0.1 % intubation team • Next wave ??
New concept ! • HCW first, Patient next • Traffic Control • Myth of negative pressure
Introduction • The health officials shut down and quarantine the hospital to control nosocomial transmission. • More than one thousand persons afected, chaos and panic rapidly ensued within the hospital. • The president of Taiwan made an executive decision to evacuate the hospital within 36 hours.
METHODS • Renovation of hospitals • A hospital: 67 beds • B hospital: 18 beds • Comparison Hospitals • 746 NPIRs
Hospital A, 松山 • The first floor is an admission office that has a special pathway which leads the patient directly to the elevator • The third floor is designated ward for suspect SARS cases, the fourth floor is for probable or confirmed cases.
Hospital A, 松山 • A residential apartment within 2 meters to the east. • A “negative-pressure like” environment • all windows due east were sealed air tight. • A 16-inchexhaust fan was installed in patient’s rooms due west. • All doors/bottom gap of patient’s rooms were sealed.
Hospital A, 松山 • The exits and staircase of each floor was sealed to prevent air interflow between floors. • A separate central air conditioning system was used to circulate air within each floor with 50% of air-exchange rate. • All of the exhaust air to the west was blow to a 60 by 30 meters restricted area,
Hospital B, 松德 • a 4-story healthcare facility for patients with tbc / chronic diseases. • the first floor is the admission office with a special pathway to the elevator. • The second floor is an 18-bed patient ward innegative pressure isolated room (NPIR).
The path to elevator was isolated with wooden/acrylic boards to differentiate the pathways for patients from the HCWs.
There is a separate entrance/exit for each HCW to enter/leave the ward to avoid crossing or overlapping with the traffic of contamination zone that the patients have passed through.
Each zone was clearly designated by wooden/plastic barriers • To avoid casual breakthrough byany directly passing and contactingfrom contaminated zones into clean zones. • Each nurse’s station was shielded with transparent plastic shield to prevent interchange of material between nurse’s station (clean zone) and the hallway (intermediate zone)
Zone of Protection • biochemical warfare • clear zone inter-zone contamination • Enter with PPE, leaving with Decontamination
Checkpoint Hand washing • Before entering/leaving each patient’s room, to prevent any contact transmission from the gloves to the knob, HCWs were required to disinfect their hands. • After entering/leaving the room and door was closed, their hands were again disinfected for protection of the next procedure. • Disinfect-Touch-Disinfect was enforced in all zones.
Traffic into Hospital • Case mix and contact transmission inside ER • A “triage and dispatch” station is located outside the hospitals.
Traffic Control • Zone of Protection • Checkpoint hand washing • Traffic into Hospital
Result • During the study period, 462 HCWs including 85 physicians, 295 nurses, and 82 administrative personnel and volunteers were clinically evaluated for SARS in study hospitals. • 2 nurses contracted SARS, PCR (+)
Using Traffic Control Strategy During Outbreak Control to Minimize Nosocomial Infection of SARS Among Health-Care Workers • Test Hospital Comparison H Hospitals • Bed A (67) B (18) Total (85) (746) • Suspected 0 (0 %)* 0 (0 %) 0 ( 0%) 43 (5.76 %) • Probable 2 (2.98 %) 0 (0 %) 2 (2.35 %) 50 (6.70 %) • Total** 2 (2.98 %) 0 (0 %) 2 (2.35 %) 93 (12.47 %) • * SARS case divided by number of patient bed • ** p = 0.004, Chi square, Fisher exact test Muh-Yong Yen, et al. 2003
PPE Respiratory contact NPIR Traffic control
Discussion • Given that PPE and NPIR are tested and available throughout Taiwan, we postulated that PPE and NPIR appear to be unsatisfactory for preventing HCWs from contracting SARS virus if the standard operative procedure was not adherent strictly, which was notunusual in the time of outbreak.
Discussion • We suspect that HCWs especially those of inadequately trained cleaner, part-time workers, may still acquire the SARS virus through inappropriate donning or removal of PPE and accidentally transmitted the virus by hands afterwards.
Discussion • “Traffic Control” differentiates the pathways of patients and the HCWs within the hospital with barriers so that each pathway may not be casually overlapping or crossing, casual contamination will than be blocked. • the integrated checkpoint hand washing spots are mandatory to be accessiblethroughout the hospital.
Discussion • the checkpoint hand washing within trafficline may strengthen the adherence and to increase frequency of hand washing. • when working in the restricted traffic control area with physical barrier, HCWs/part-time workers will upraise their consciousness to a surroundings of self-control and discipline and to a highest grade infection control standard.
Discussion • our data suggest that probable or suspect SARS case patients may not need to be housed in standard NPIRs for their entire stay. • For stablized patients which indicate that the viral load of contamination is mild. • They may be placed in a step-down regular wards with minor renovation and traffic control instituted.
Using Traffic Control Strategy During Outbreak Control to Minimize Nosocomial Infection of SARS Among Health-Care Workers • Test Hospital Comparison Hospitals PMH • Bed Total (85) (746) (580) • Total** 2 (2.4 %) 93 (12.5 %) 62 (10.7 %) • HCW 0.5 % / 0*** 2.0 % • * SARS case divided by number of patient bed • ** p = 0.004, Chi square, Fisher exact test • *** SARS hospital (松山 三重) Muh-Yong Yen, et al. 2003
The End Thanks for your attention



![[M2] Traffic Control](https://cdn2.slideserve.com/4578602/m2-traffic-control-dt.jpg)