PERICARDIAL DISEASES
PERICARDIAL DISEASES. GENERAL CONSIDERATIONS. The pericardium consists of two layers: the inner visceral layer, which is attached to the epicardium , and an outer parietal layer. About 50 mL of serous fluid is normally present and provides lubrication between the two layers.

PERICARDIAL DISEASES
E N D
Presentation Transcript
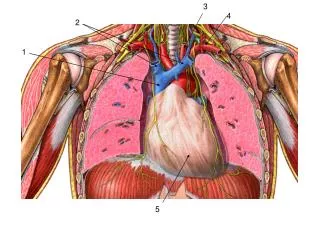
GENERAL CONSIDERATIONS • The pericardium consists of two layers: the inner visceral layer, which is attached to the epicardium, and an outer parietal layer. • About 50 mL of serous fluid is normally present and provides lubrication between the two layers. • The pericardial reflection encompasses the heart and great vessels. • The pericardium stabilizes the heart in anatomic position and reduces contact between the heart and the surrounding structures. • It is composed of fibrous tissue and although it will permit moderate changes in cardiac size, it cannot stretch rapidly enough to accommodate rapid dilation of the heart or accumulation of fluid without increasing intrapericardial (and, therefore, intracardiac) pressure. • The pericardium is often involved by processes that affect the heart, but it may also be affected by diseases of adjacent tissues and may itself be a primary site of disease.
Physiology of the pericardium • The normal pericardium is not essential to life: the pericardial space is often obliterated after open heart surgery and both layers may be removed in patients with constrictive pericarditis without apparent ill effect. • Whether restraint by the normal pericardium is of any pathophysiological importance as a mechanism limiting stroke volume in disease remains uncertain.
Acquired pericardial disease • Diseases of the pericardium may be considered from two points of view. • The first is etiological, the second is in terms of the physiological and clinical disturbances that result. • There is no fixed relation between the two, so that an account will be given of the different diseases affecting the pericardium and then of the three main syndromes: acute pericarditis, pericardial tamponade and pericardial constriction.
Pericarditis • Pericarditis is a condition in which the sac-like covering around the heart (pericardium) becomes inflamed.
Pericarditis and cardiac tamponade involve the potential space surrounding the heart or pericardium. Pericarditis is one cause of fluid accumulation in this potential space and cardiac tamponade is the hemodynamic result of fluid accumulation.
Who gets pericarditis and what does it feel like? • This problem occurs most often in men ages 20 to 50. • Chest pain is common, especially pain behind the breastbone. Sometimes this pain spreads to the neck and left shoulder. • Pain from pericarditis is different from angina. Angina feels like pressure, but pericarditis usually is a sharp, piercing pain over the center or left side of the chest. Often this pain gets worse if the person takes a deep breath. Less often the pain is dull. • A fever is also common. • Often people with pericarditis report feeling sick. • Some have pain when they swallow.
Acute pericarditis • By far the most common pathologic process involving the pericardium. • May be classified both clinically and etiologically. • Acute (< 2 weeks) inflammation of the pericardium may be infectious in origin or may be due to systemic diseases (autoimmune syndromes, uremia), neoplasm, radiation, drug toxicity, hemopericardium, postcardiac surgery or contiguous inflammatory processes in the myocardium or lung.
Acute pericarditis • Incidence – Post mortem 1-6%, diagnosed in only 0.1% of hospitalized patients. 5% of patients seen in emergency rooms with CP and no MI. • Sequelae – Cardiac tamponade Recurrent pericarditis Pericardial constriction
Etiology • Viral or idiopathic • After MI • Infectious diseases • With dissecting aortic aneurysms • Trauma • Metastasis • XRT • Uremia • After cardiac or other thoracic surgery • Autoimmune diseases • Medications
Viral infections • especially infections with coxsackieviruses and echoviruses but also influenza, Epstein–Barr, varicella, hepatitis, mumps and HIV viruses are the most common cause of acute pericarditis and probably are responsible for many cases classified as idiopathic. • Males—usually under age 50 years—are most commonly affected. • The differential diagnosis is primarily with myocardial infarction.
Tuberculouspericarditis • has become rare in developed countries but remains common in other areas • It results from direct lymphatic or hematogenous spread; clinical pulmonary involvement may be absent or minor, although associated pleural effusions are common.
Bacterial pericarditis • has become rare and usually results from direct extension from pulmonary infections • Pneumococci can cause a primary pericardial infection. • Borreliaburgdorferi, the organism responsible for Lyme disease, can also cause myopericarditis.
Uremic pericarditis • is a common complication of renal failure • the pathogenesis is uncertain • it occurs both with untreated uremia and in otherwise stable dialysis patients
Neoplasticpericarditis • Spread of adjacent lung cancer as well as invasion by breast cancer, renal cell carcinoma, Hodgkin disease and lymphomas are the most common neoplastic processes involving the pericardium and have become the most frequent causes of pericardial tamponade in many countries.
Dressler syndrome • Pericarditis may occur 2–5 days after infarction due to an inflammatory reaction to transmural myocardial necrosis postmyocardial infarction or postcardiotomypericarditis .
Post-radiotherapy pericarditis • Radiation can initiate a fibrinous and fibrotic process in the pericardium, presenting as subacutepericarditis or constriction. • Radiation pericarditis usually follows treatments of more than 4000 cGy delivered to ports including more than 30% of the heart.
Other causes of pericarditis • connective tissue diseases, such as lupus erythematosus and rheumatoid arthritis • drug-induced pericarditis (minoxidil, penicillins) • myxedema
Clinical presentation • History • Physical exam - 85% have audible friction rub during the course of their disease ( the rub is high pitched scratchy or squeaky sound best heard at the left sternal border at end of expiration with the patient leaning forward) • The rub has three components- atrial systole, ventricular systole and rapid ventricular filling during early diastole.
Symptoms and Signs • The presentation and course of inflammatory pericarditis depend on its cause, but all syndromes are often (not always) associated with chest pain, which is usually pleuritic and postural (relieved by sitting). • The pain is substernal but may radiate to the neck, shoulders, back or epigastrium. • Dyspnea may also be present and the patient is often febrile. • A pericardial friction rub is characteristic , with or without evidence of fluid accumulation or constriction
Clinical findings • There are three main components to the clinical syndrome of acute pericarditis: • chest pain • pericardial rub • ECG changes
Chest pain • The pain is usually retrosternal, continuous and sharp or 'raw' in character. • It is frequently aggravated by sudden movements or deep inspiration and is relieved by sitting up. • Less commonly it may resemble angina pectoris, or may be mild and 'atypical'. • Painful breathing causes dyspnoea. • The onset of the pain is usually sudden, but in idiopathic pericarditis, it may have been preceded by several days' malaise or other non-specific symptoms.
Pericardial pain • Characteristically, however, pericardial pain may be relieved by sitting up and leaning forward and is intensified by lying supine.
Pericardial friction rub • the most important physical sign of acute pericarditis • may have up to three components per cardiac cycle • high-pitched, scratching and grating • it is heard most frequently during expiration with the patient in an upright and leaning forward position • the rub is often inconstant and the loud to-and-fro leathery sound may disappear within a few hours, possibly to reappear the following day
Tuberculouspericarditis • The presentation tends to be subacute, but nonspecific symptoms (fever, night sweats, fatigue) may be present for days to months. • Pericardial involvement develops in 1–8% of patients with pulmonary tuberculosis.
Bacterial pericarditis • Symptoms and signs are similar to those of other types of inflammatory pericarditides, but patients appear toxic and are often critically ill.
Uremic pericarditis • can present with or without symptoms • fever is absent
Neoplasticpericarditis • often is painless • the presenting symptoms relate to hemodynamic compromise or the primary disease
Postmyocardial infarction or postcardiotomypericarditis (Dressler syndrome) • Usually presents as a recurrence of pain with pleural-pericardial features • A rub is often audible, and repolarization changes on the ECG may be confused with ischemia. • Large effusions are uncommon and spontaneous resolution usually occurs in a few days. • Dressler syndrome occurs weeks to several months after myocardial infarction or open heart surgery, may be recurrent and probably represents an autoimmune syndrome. • Patients present with typical pain, fever, malaise and leukocytosis. • Rarely, other symptoms of an autoimmune disorder, such as joint pain and fever, may occur. • Tamponade is rare with Dressler syndrome after myocardial infarction but not when it occurs postoperatively.
Radiation pericarditis • The clinical onset is usually within the first year but may be delayed for many years.
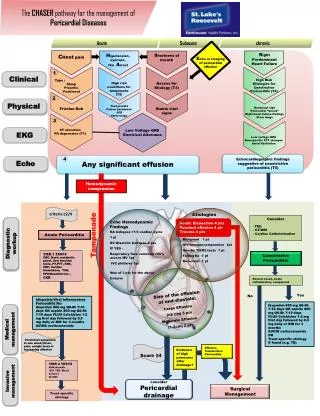
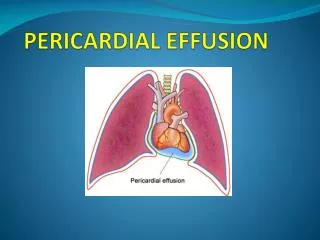
PERICARDIAL EFFUSION • Pericardial effusion can develop during any of the processes previously discussed. • The speed of accumulation determines the physiologic importance of the effusion. • Because the pericardium stretches, large effusions (> 1000 mL) that develop slowly may produce no hemodynamic effects. Conversely, smaller effusions that appear rapidly can cause tamponade. • Tamponade is characterized by elevated intrapericardial pressure (> 15 mm Hg), which restricts venous return and ventricular filling. As a result, the stroke volume and pulse pressure fall and the heart rate and venous pressure rise. Shock and death may result.
Pericardial effusion • Differentiation from cardiac enlargement may be difficult on physical examination, but heart sounds tend to become faint with pericardial effusion; the friction rub may disappear and the apex impulse may vanish, but sometimes it remains palpable, albeit medial to the left border of cardiac dullness. • The base of the left lung may be compressed by pericardial fluid, producing Ewart’s sign, a patch of dullness beneath the angle of the left scapula. • The chest roentgenogram may show a “water bottle” configuration of the cardiac silhouette, but may also be normal or almost so.
Symptoms • Pericardial effusions may be associated with pain if they occur as part of an acute inflammatory process or may be painless, as is often the case with neoplastic or uremic effusion. • Dyspnea and cough are common, especially with tamponade. • Other symptoms may result from the primary disease.
SIGNS • A pericardial friction rub may be present even with large effusions . • In cardiac tamponade, tachycardia, tachypnea, a narrow pulse pressure and a relatively preserved systolic pressure are characteristic. • Pulsusparadoxus—a greater than 10 mm Hg decline in systolic pressure during inspiration due to further impairment of LV filling—is the classic finding, but it may also occur with obstructive lung disease. • Central venous pressure is elevated and there is no evident y descent in the RA, RV or LV hemodynamic tracings. • Edema or ascites are rarely present; these signs favor a more chronic process.
Investigations • Electrocardiogram • Chest X-ray • Echocardiography
ECG • in acute pericarditis without massive effusion usually displays changes secondary to acute subepicardialinflammation • usually there are no significant changes in QRS complexes, except for some reduction in voltage in patients with large pericardial effusions • elevation of the ST segments, often with upward concavity, involving two or three standard limb leads and V2 to V6, with reciprocal depressions only in aVR and sometimes V
EKG • Stages of pericarditis: I- Diffuse ST elevation and PR segment depression (seen in more than 80%) II- Normalization of the ST and PR III- Widespread T- wave inversions IV- Normalization of the T waves • The most reliable distinguishing feature may be the ratio of ST segment elevation (in millimeters) to T-wave amplitude in lead V6; ratio > 0.24
This 12-lead electrocardiogram is representative of pericarditis. Stage 1 electrocardiograph changes in a patient with acute pericarditis. Stage 2 ECG changes in patient with acute pericarditis obtained 3 days into clinical course.
ECG criteria: • ACUTE PERICARDITIS: • Concave (saddle-shaped) ST segment elevation; • ST may be normal or nonspecific (10% cases). • PERICARDIAL EFFUSION: • Low voltage QRS complexes; • Alternating QRS morphologies (electrical alternans). • CONSTRICTIVE PERICARDITIS: • Large T wave and bifid; • Low voltage QRS complexes; • ST plan, isoelectric or depressed. • CARDIAC TAMPONADE: • Low voltage QRS complexes; • Electrical alternans.
Chest X-ray • may suggest enlargement of heart tissue and can be used to rule out other problems within the chest
Chest radiographs revealing markedly enlarged cardiac silhouette and normal-appearing lung parenchyma in prepericardiocentesis (A) and postpericardiocentesis (B).
Echo • The cardiologist looks for the presence of fluid in the pericardial sac, although in many mild cases of acute pericarditis, there is no pericardial fluid seen with echocardiography.
This ultrasonogram demonstrates a normal subcostal 4-chamber view of the heart. The pericardium is brightly reflective (echogenic or white in appearance). LA = left atrium; LV = left ventricle; RA = right atrium; RV = right ventricle. This is a modified subcostalultrasonographic view of the heart in which a thick anechoic (dark or black) stripe is seen surrounding the heart (H). The stripe represents a large amount of fluid (F) in the pericardium, indicating tamponade.