Download
1 / 13
130 likes | 286 Vues
Variations in Quality Outcomes Among Hospitals in Different Types of Health Systems, 1995 - 2000. Askar Chukmaitov, M.D., M.P.A. Virginia Commonwealth University Gloria J. Bazzoli, Ph.D. Virginia Commonwealth University. Agency For Healthcare Research and Quality, Grant #R01 HS13094.

E N D
Variations in Quality Outcomes Among Hospitals in Different Types of Health Systems, 1995 - 2000 Askar Chukmaitov, M.D., M.P.A. Virginia Commonwealth University Gloria J. Bazzoli, Ph.D. Virginia Commonwealth University Agency For Healthcare Research and Quality, Grant #R01 HS13094
Rationale for the Study • Forces to reduce costs and improve quality of care motivated hospitals to join health systems in the 1990s • Bazzoli et al. (2000) have found differences in costs and financial performance across hospital system types • Did not examine hospitals’ quality performance across different types of hospital systems • Important issue given concerns regarding safety and quality • 44,000 to 98,000 hospital deaths in the US each year caused by medical errors (IOM, 1999)
Methods • Design • Longitudinal analysis of 1995-2000 data • Data: • AHA, HCUP (SID) 1995-2000 • Sampling • All nonfederal, short-term, general medical-surgical hospitals from 11 states (AZ, CA, CO, FL, IA, MD, MA, NJ, NY, WA, and WI) • Analytic Approach • Adjusted Least Square Means (ALSM) calculated for each IQI and PSI: • Patient age, gender, acuity, and case-mix
Key Variables • Hospitals in Different Types of Health Systems: • Centralized Health System (CHS), Centralized Physician/Insurance Health System, Moderately Centralized Health System (MCHS), Decentralized Health System (DHS), Independent Hospital System (IndHS) (Bazzoli et al. 1999) • Patient Outcomes: • IQIs are measures of mortality rates for specific diagnosis; • IQIs selected for study: AMI, CHF, Stroke, GI hemorrhage, and Pneumonia • PSIs are adverse events or complications that occur during care; • Selected PSIs: complications of anesthesia, death in low mortality DRGs, decubitus ulcer, infections due to medical care, post-op hemorrhage, post-op PE and DVT, sepsis, and accidental puncture and laceration
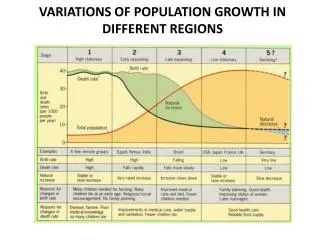
Description of Various Types of Health Systems (Bazzoli et al. 1999)
Results for Different System Types • IQI mortality rates for AMI, CHF, Stroke, GI hemorrhage, and Pneumonia: • The best performers – hospitals in DHS, CHS, and CPIHS in the 1995 – 2000 period • Significantly better than hospitals in other system types • PSI adverse event rates: • Less clear and less significant trends for the best or the worse performers • However, hospitals in more centralized health systems tend to perform worse than hospitals in other system types for a number of PSIs
Results Results for Different System Types Results
Results for IQI and PSI Indicators Over Time • Increase in IQI mortality rates outcomes after 1998, except AMI • Leveling or increase in PSI adverse events after 1998
Significance to Policy • Hospitals in more centralized health systems and in Decentralized Health Systems have better IQIs than hospitals in other systems. This relationship holds over time. • Hospitals in more centralized health systems tend to perform worse in terms of PSI, even though differences are not always significant. • Future research needs to examine the organizational characteristics and internal processes adopted by different systems that lead to higher quality of care as measured by IQI and PSI performance. • Performance on many indicators declined after 1998 – suggestive of BBA effect. • Future research needs to look for potential adverse quality effects from BBA or potentially other market/policy factors.