Voluntary HIV Testing in New Jersey Emergency Departments: Enhancing Early Detection and Care
This study evaluates the implementation of voluntary HIV testing in New Jersey hospital emergency departments (EDs) to identify undiagnosed HIV cases. Despite advancements in treatment, late-stage diagnoses remain prevalent. The testing program aims to connect at-risk populations, particularly minorities and younger adults, to necessary services and improve overall health outcomes. Findings indicate high seroprevalence rates and a lack of awareness among HIV-positive individuals, underscoring the importance of continued screening efforts in ED settings to reduce the number of undiagnosed cases.

Voluntary HIV Testing in New Jersey Emergency Departments: Enhancing Early Detection and Care
E N D
Presentation Transcript
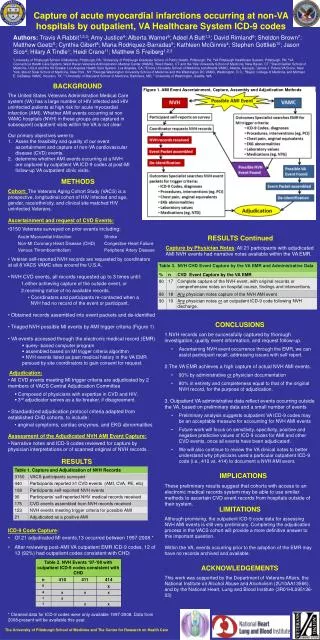
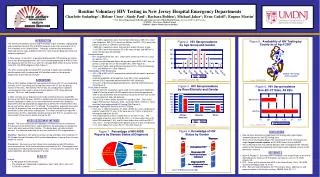
Routine Voluntary HIV Testing in New Jersey Hospital Emergency Departments Charlotte Sadashige1; Helene Cross1; Sindy Paul1; Barbara Bolden1; Michael Jaker2; Evan Cadoff3; Eugene Martin3 1 New Jersey Department of Health and Senior Services, Public Health Branch, Division of HIV/AIDS Services 2 UMDNJ - New Jersey Medical School 3 UMDNJ - Robert Wood Johnson Medical INTRODUCTION The Centers for Disease Control and Prevention (CDC) estimates undiagnosed and unreported cases of HIV and AIDS comprise more than one-quarter of all HIV infections in the United States.1 Although, treatment has dramatically improved survival rates of patients with HIV, rates of earlier diagnosis have only modestly improved.2 In New Jersey, at least 40% of persons diagnosed with HIV disease are tested late in their disease progression; 30% have already progressed to AIDS at their first diagnosis with the HIV virus; and 12% develop AIDS within one year of their initial HIV (not AIDS) diagnosis (See Figure 1). The CDC recommends increased HIV screening in health care settings to identify persons with unrecognized HIV infection earlier in their disease progression to link them to services.3 BACKGROUND Prior to 2002, publicly-funded HIV counseling and testing (HIV CT) was conducted primarily at HIV Counseling and Testing Sites where HIV CT was the primary function of the clinic. Alternatively, HIV CT was also conducted at traditional service-specific clinics such as drug treatment centers, STD, family planning, prenatal, TB clinics, and through outreach. In 2002, the New Jersey Department of Health and Senior Services (NJDHSS), Division of HIV/AIDS Services (DHAS) in collaboration with University Hospital (UH) Newark conducted a needs assessment to determine whether the Emergency Department (ED) would provide an opportunity to identify HIV-infected clients who do not visit facilities where HIV CT is offered. These patients, especially those who use the ED for primary care, are the most likely to fall through the cracks of the prevention system and remain undiagnosed. The recent availability of rapid HIV testing makes the ED a logistically feasible setting to offer HIV CT, as patients may receive their HIV test results before leaving the ED. NEEDS ASSESSMENT METHODS Design: The assessment used an Anonymous Unlinked Survey to estimate the HIV prevalence rate of ED clients, and to determine the percentage of seropositive clients who were aware of their infection. The design does not require patient consent. It is unbiased and yields the only true estimate of HIV seroprevalence. Eligibility: Specimens from patients 18 years of age and older who visited the UH ED October through December 2002 and had blood drawn as part of their visit were eligible for testing. Procedures: Remnant sera from clinical tests conducted on adult ED patients were recovered from UH’s clinical laboratory and tested for HIV. Demographic and clinical data were abstracted from medical charts. All links between specimens and patient identifiers were destroyed prior to testing. • 2,174 (68%) specimens were from African-Americans, 339 (10%) were from Hispanics, 308 (10%) were from Whites, and 372 (12%) were from persons of other or unknown race/ethnicity • 1,088 (34%) specimens were from persons under 35 years of age, 1,120 (35%) were from persons 35 to 50 years of age, and 985 (31%) were from persons 50 and older • Seroprevalence • HIV seroprevalence was 10%. Rates were similar for men (11%) and for women (10%). • Rates were considerably higher for persons ages 35-49 (18%) than for persons under 35 (6%) or 50 and older (6%) (See Figure 2). • Rates were higher among African Americans (13%) than for Hispanics (7%), and Whites (4%) (See Figure 3). • Knowledge of HIV Serostatus • 40% (198 of 332) of HIV-seropositive patients did not report a previous diagnosis • A greater proportion of seropositive men (46%) than seropositive women (35%) reportedly did not know their HIV serostatus. • Only 24% of previously diagnosed patients reported antiretroviral use (See Figure 4). • From Data to Action • Results from the assessment were used as the rationale to implement rapid HIV testing of adult UH ED patients when clinically appropriate, when it will not interfere with the primary reason for the ED visit, or with an assessment of high risk behavior. • The first ED in New Jersey started HIV testing in 2004. The UH ED began HIV testing in February 2005. As of April 2007, 22 EDs in 13 NJ counties have implemented HIV testing (See Figure 5). • Percentage Testing HIV Positive at HIV CT Sites • From July 1, 2006 to December 31, 2006, 38,933 tests were conducted at publicly funded HIV CT sites; 3,750 were done at 21 EDs, of which 634 were performed at the UH ED. • The seroprevalence at EDs is higher than at non-ED CT sites. The percentage of positive tests at UH ED (5.4%) is 3 times higher than at 20 other EDs combined (1.8%), and 5.4 times higher than at all non-ED CT sites (1.0%). The percentage of HIV positive tests at all EDs including UH is 2.4 times higher than at non-ED CT sites (See Figure 6). CONCLUSIONS • New Jersey’s Emergency Department HIV testing sites report higher seroprevalence than non-ED testing sites. • Since University Hospital began HIV screening in the ED, UH became the single largest volume reporter of HIV/AIDS cases to the NJDHSS. • HIV screening in EDs may identify persons with unrecognized HIV infection earlier in their disease progression and may broaden patients’ access to HIV prevention and care. • REFERENCES 1.Glynn M, Rhodes P. Estimated HIV Prevalence in the United States at the end of 2003 [Abstract]. National HIV Prevention Conference, June 12-15, 2005; Atlanta, GA. 2. CDC. Cases of HIV infection and AIDS in the United States, 2004. HIV/AIDS Surveillance Report 2005; 16:16-45. 3. CDC. Revised recommendations for HIV testing of adults, adolescents, and pregnant women in health-care settings. MMWR 2006; 55:1-17. • RESULTS • Sample • 3,193 specimens were tested • The sample was comprised of specimens from 1,623 (50%) men and 1,570 (49%) women