Download
1 / 15
150 likes | 263 Vues
This overview explores the hierarchical structure of motor control in the brain, detailing high-level planning and execution strategies involving the cortex, basal ganglia, motor cortex, and cerebellum. It explains pathways like the lateral and ventromedial pathways, which manage distal and proximal muscles respectively. The role of premotor areas and the "go" signal from the basal ganglia is highlighted, alongside the influence of disorders such as Parkinson’s and Huntington’s diseases on movement control. Finally, it discusses how the cerebellum refines motor actions for accuracy and coordination.

E N D
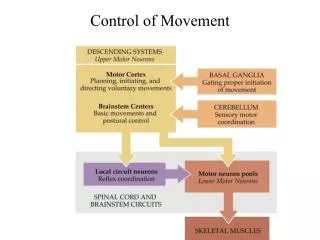
Motor Control Hierarchy • High level – plans and executes strategy • Association areas of cortex • Basal ganglia gives the “go” signal • Middle level – develops tactics • Motor cortex • Cerebellum • Low level – executes movement • Brain stem, spinal cord
Two Pathways to the Brain • Two pathways: • Lateral pathway • Ventromedial pathway • Lateral pathways control fractionated movement of distal muscles, especially flexors, under direct cortical control: • Corticospinal – new, originates in motor cortex • Rubrospinal – old, originates in red nucleus of midbrain
Ventromedial Pathways • Four pathways control proximal & axial muscles. • Vestibulospinal – maintains stability of head and turns it, maintains upright posture & balance • Input from labyrinth of inner ear • Tectospinal – orients eyes (fovea) on image • Receives input from superior colliculus • Pontine – resists gravity and maintains posture • Medullary – liberates muscles from anti-gravity control
Voluntary Movement • Involves almost all of the cortex. • Goal-directed movement depends on: • Knowing where the body is in space. • Knowing where it wants to go. • Selection of a plan to get it there. • Once a plan is devised, it must be kept in memory until it can be executed. • Instructions to implement the plan must be issued. • These functions are localized to different areas.
Parts of the Motor System • Premotor areas (PMA, SMA) – plan the motor activity • Primary motor cortex (M1) – initiates motor activity: • Basal ganglia loop (near thalamus) gives the “go” signal • Cerebellar loop – tells the motor cortex how to carry out the planned activity • Controls direction, timing and force by activating populations of motor neurons in learned programs.
Planning Movement • Goal directed movement involves many cortical areas that communicate with Area 6 in Frontal lobe. • Area 6 has two parts: • PMA (premotor area) • SMA (supplemental motor area) – lesions produce apraxia (impaired complex acts) • Area 6 plans an action and stays active until it is executed (“go” signal).
The “Go” Signal • Area 6 receives a “Go” signal from the thalamus (VLo). • Input to the thalamus comes from the basal ganglia deep in subcortical areas. • A circuit through the basal ganglia inhibits excitation of the SMA by VL. • Inhibition is released by the substantia nigra, permitting VL to send a “go” signal to the SMA.
Disorders of Movement • Hypokinesia – a lack of movement caused by increased inhibition of the thalamus by the basal ganglia. • Hyperkinesia – too much movement caused by decreased basal ganglia input, removing inhibition of the thalamus. • Bradykinesia – slowness of movement. • Akinesia – difficulty initiating movement.
Parkinson’s Disease • Caused by degeneration of the substantia nigra and depletion of dopamine. • Impairs the “go” signal circuit to VLo & SMA. • Symptoms are bradykinesia, akinesia, increased muscle tone (rigidity), tremors of hands and jaw, especially at rest. • Treated by the drug L-Dopa, the precursor to dopamine.
Huntington’s Disease • Hereditary, progressive, lethal syndrome caused by loss of neurons in the basal ganglia, cortex, and elsewhere. • Symptoms are hyperkinesia, dyskinesia (abnormal movement), dementia (impaired cognition), and personality disorders. • Chorea – uncontrolled and purposeless movement with rapid, irregular flow and flicking motions.
Ballism • Caused by damage or lesions to the basal ganglia, usually resulting from stroke. • Loss of excitation of the global pallidus (normally inhibiting VLo) results in too much excitation of SMA. • Symptoms are violent, flinging movements of the extremities.
Coding the Direction of Movement • Motor cortex (M1) neurons fire at different rates depending on the desired direction. • Firing rates are averaged across populations of M1 neurons. • When contributing neurons are inhibited, resultant direction changes. • Cerebellum controls sequence.
Cerebellum • Creates a detailed sequence of precisely timed muscle contractions needed to execute movement. • Ataxia – uncoordinated, inaccurate movement. • Dyssynergia – decomposition of synergistic muscle movements. • Dysmetric – imprecise movement, overshooting or undershooting target. • Alcohol impairs cerebellar functioning.
Cerebellar Motor Loop • Cerebellum supplies input to the motor cortex via the pons (pontine nuclei) and area VLc of the thalamus. • Feedback from the sensory cortex guides activity of the cerebellum to create and store learned programs of movement. • Cerebellum compares what was intended with what happened, then modifies circuits to compensate.