The Respiratory System
The Respiratory System. Anatomy and Mechanics. Pulmonary volumes and capacities (a capacity is the sum of two or more volumes). The system can be divided into conducting and respiratory zones.

The Respiratory System
E N D
Presentation Transcript
The Respiratory System Anatomy and Mechanics
Pulmonary volumes and capacities(a capacity is the sum of two or more volumes)
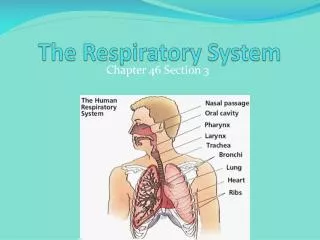
The system can be divided into conducting and respiratory zones The airway undergoes about 16 generations of branching between trachea and respiratory bronchioles. This is a situation where each generation of branches has a lower flow resistance than the previous one. The basic functional unit of the lung is an acinus (pl. acini) – a group of alveoli served by a single terminal bronchiole. Each alveolus is a thin-walled sac that is densely surrounded by pulmonary capillaries.
The airway is under autonomic control • The airway is lined with smooth muscle that is dually innervated by the ANS: • Psymp – constricts • Symp – dilates However, other chemical mediators may play important roles, including prostaglandins and NO
The thoracic cavity is a box whose volume changes over the respiratory cycle The thoracic cavity is a box with one opening – the thoracic outlet - through which the trachea passes to connect the lungs with the atmosphere. The volume of the box can be increased by contraction of the external intercostals, which lift the ribs and swing them outward, and by contraction of the diaphragm, which takes a domed shape when relaxed and a flatter shape when contracted.
Lung-Chest Mechanics Intrapleural fluid connects lung and chest wall – the two opposing forces of chest elastic recoil and lung elastic recoil cause intrapleural pressure to be negative relative to atmospheric pressure. The coupling ensures that the lungs do not collapse at any stage of the respiratory cycle. When respiratory muscles are relaxed, the tendency of the chest wall to spring out is balanced by the tendency of the lung to collapse. If the two elastic components become uncoupled, as when the chest wall is breached, the lung collapses and the chest wall springs out. The chest wall elastic recoil can be thought of as a stiff spring that wants to pull the chest out The lung elastic recoil is a relatively weak spring that wants to collapse the lung on itself.
Pulmonary surfactant • The major source of lung elastic recoil is the surface tension of the thin layer of water on the alveolar surface • If the water were pure, there would be two bad consequences • Inflating the lung against the resistance of the surface tension would require a lot of effort, and respiratory work would be much greater • Small alveoli would tend to merge into larger ones, reducing lung surface area These problems are prevented by pulmonary surfactant, a phospholipid detergent secreted by type B alveolar cells.
How surfactant preserves the froth-like structure of the lung Without surfactant, large alveoli have smaller pressures than smaller ones and tend to grow at the expense of small ones With surfactant, large alveoli tend to become smaller and smaller ones tend to become larger
Lack of surfactant causes respiratory distress syndromes • Premature infants: ordinarily a rise in levels of the adrenal cortical hormone cortisol induces production of surfactant before birth. • In some adults with lung trauma from smoke inhalation or toxic gas, surfactant production is impaired
Pressure and volume changes over the respiratory cycle Note that pressure changes at the level of the alveoli are what drive movement of air in ventilation – alveolar pressure is negative to atmospheric during inspiration and positive during expiration. In contrast, intrapleural pressures are always negative and simply become more negative as the chest is expanded during inspiration.
Some thought questions • What changes would you expect in the intrapleural pressure values in the case of each of the following: • Increased ventilation during exercise • An increase in airway resistance, as in asthma • A decrease in lung compliance (i.e. an increase in stiffness), as in respiratory distress syndrome or fibrotic lung disease?
Well, don’t say I never give anything away… This is the answer to the first thought question, showing a TV of 500 ml and one of 1000 ml The next slide should help some with questions 2 and 3
Respiratory work can be divided into two components: elastic work and flow resistance work The alveolar pressure trace reflects only the force needed to move a tidal volume of air – overcoming the flow resistance of the airway The intrapleural pressure trace includes both the flow-resistive component and an additional one – the force needed to overcome the lung’s elastic recoil.
1-second forced expiratory volume Classically, FEV1.0 was used as a one measure of lung health – currently, the maximum flow velocity a patient can achieve during an expiration is used, because it is simpler to measure and can be done by patients with an at-home device.
Another thought question or two… • How would FEV1.0 (or peak flow velocity) change with an increase in airway resistance, as with asthma? How about with an increase in lung compliance, as in emphysema? Or a decrease in lung compliance, as in fibrotic disease or respiratory distress syndrome?
Alright, now I’m giving away the whole candy store… emphysema asthma Pulmonary edema
System ventilation, alveolar ventilation and deadspace ventilation • System: Vtotal =TV x RR – about 5 L/min at rest • Alveolar: Valv = (TV – DSV) x RR What is dead space and why does it matter? This is the volume of the airway that must be ventilated in order to bring air to the alveoli. Anatomically, it corresponds to the entire conducting system. At the end of an expiration, the last of the gas that leaves the alveoli passes into the conducting system. This gas then is the first to enter the alveoli in the next inspiration. Thus, for all practical purposes, this dead space gas never left the alveoli and could not contribute to alveolar ventilation during the next breath. Similarly, air from the atmosphere that was drawn into the conducting system at the end of an inspiration simply is returned to the atmosphere at the beginning of the next expiration without ever reaching the alveoli.
Alveolar ventilation vs pulmonary volume DS ventilation is about 25-30% of system ventilation at rest. For a person whose respiratory rate is 12 breaths/min, dead space volume is 150 ml and tidal volume is 500 ml, Valv is 4200 ml/min. This sounds like a nice large number. However, for a single breath of 500 ml, with 350 ml of actual alveolar ventilation, the 350 ml is added to a lung volume (the functional residual volume) that is already 2300 ml. As a result of this, a single breath has very little impact on the composition of alveolar gas, and alveolar gas will always have a lower O2 content and a higher CO2 content than atmospheric air.
Ventilation overbalances perfusion Alveolar ventilation and perfusion are regulated at the level of single acini Pulmonary arterioles respond to changes in oxygen and carbon dioxide exactly the opposite of the way systemic ones do. Bronchioles constrict in response to decreased carbon dioxide and increased oxygen - they dilate when the opposite changes occur. These responses tend to optimize the ventilation/perfusion ratio throughout the lung. Perfusion overbalances ventilation