Download
1 / 34
340 likes | 468 Vues
CYCLING MULTI-KINASE INHIBITORS IN IMATINIB-RESISTANT GASTROINTESTINAL STROMAL TUMORS TO MAXIMIZE DISEASE CONTROL: PRECLINICAL AND CLINICAL RATIONALE. César Serrano, Grant Eilers , Meijun Zhu, Anu Gupta, George D. Demetri ,

E N D
CYCLING MULTI-KINASE INHIBITORS IN IMATINIB-RESISTANT GASTROINTESTINAL STROMAL TUMORS TO MAXIMIZE DISEASE CONTROL: PRECLINICAL AND CLINICAL RATIONALE César Serrano, Grant Eilers, MeijunZhu, AnuGupta, George D. Demetri, Suzanne George, Sebastian Bauer, Brian P. Rubin, Jonathan A. Fletcher Brigham and Women’s Hospital; Dana-Farber Cancer Institute; Harvard Medical School, Boston, MA, USA; Lerner Research Institute and Cleveland Clinic, Cleveland, OH; West German Cancer Center, Essen, Germany CTOS 18th Annual Meeting Oct 30- Nov 2, 2013 New York Paper 037
Background • KIT and PDGFRA are primary drivers of oncogenic signaling in GISTs. • KIT inhibition with tyrosine-kinase inhibitors (TKIs)improves outcomes in most GIST patients. • Resistance to TKIs eventually emerges in virtually all GIST patients. • KIT secondary resistance mutations are the main mechanism of TKI failure.
Secondary resistance in GIST SECONDARYMUTATIONS FREQUENCY ATP-binding pocket V654 40% Exon 13 Exon 14 Exon 9 Exon 11 Activation Loop D816 D820 Exon 17 30% N822 Y823 Debiec-Rychter M, 2005 Antonescu CR, 2005 Wardelmann E, 2006 Heinrich MC, 2008 Liegl B, 2008
Secondary resistance in GIST SECONDARYMUTATIONS FREQUENCY ATP-binding pocket V654 40% Exon 13 Exon 14 Exon 9 Exon 11 Activation Loop D816 D820 Exon 17 30% N822 Y823 Debiec-Rychter M, 2005 Antonescu CR, 2005 Wardelmann E, 2006 Heinrich MC, 2008 Liegl B, 2008
Secondary resistance in GIST DRUG SENSITIVITY SECONDARYMUTATIONS FREQUENCY Sunitinib Imatinib V654 40% Exon 13 Exon 14 Exon 9 Exon 11 D816 D820 Exon 17 30% N822 Y823 Sensitive Debiec-Rychter M, 2005 Antonescu CR, 2005 Wardelmann E, 2006 Heinrich MC, 2008 Liegl B, 2008 Resistant
Secondary resistance in GIST DRUG SENSITIVITY SECONDARYMUTATIONS FREQUENCY Sunitinib Imatinib V654 40% Exon 13 Exon 14 Exon 9 Exon 11 D816 D820 Exon 17 30% N822 Y823 Sensitive Debiec-Rychter M, 2005 Antonescu CR, 2005 Wardelmann E, 2006 Heinrich MC, 2008 Liegl B, 2008 Resistant
Second- and third-line treatment in GIST • Regorafenib (REGO) has recently obtained FDA-approval in GIST patients after failure of imatinib (IM) and sunitinib (SU). • There is substantial heterogeneity of secondary KIT resistant mutations between and within metastases from individual patients after progression on TKIs. • Progression-free survival after imatinib failure is 4 to 6 months irrespective of the second- or third-line TKI used.
Aims We investigated novel strategies to overcome heterogeneity of resistant clones in TKI-resistant GIST patients.
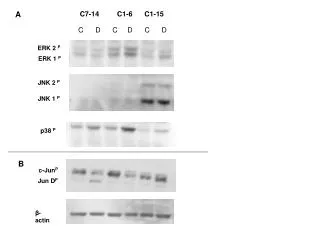
Imatinib, sunitinib and regorafenib are active against primary KIT exon 11 mutation IM REGO SU DMSO DMSO DMSO nM 50 100 500 50 100 500 50 100 500 p-KIT (Y703) p-AKT S473 p-S6 (S235/236) Actin
Imatinib, sunitinib and regorafenib are active against primary KIT exon 11 mutation IM REGO SU DMSO DMSO DMSO nM 50 100 500 50 100 500 50 100 500 p-KIT (Y703) p-AKT S473 p-S6 (S235/236) Actin
Imatinib, sunitinib and regorafenib are active against primary KIT exon 11 mutation IM REGO SU DMSO DMSO DMSO nM 50 100 500 50 100 500 50 100 500 p-KIT (Y703) p-AKT S473 p-S6 (S235/236) Actin
Sunitinib and regorafenib have complementary activity against imatinib-resistant GIST cell lines *IC50s: Green = predictive of clinical efficacy Red = predictive of clinical resistance
Sunitinib and regorafenib have complementary activity against imatinib-resistant GIST cell lines *IC50s: Green = predictive of clinical efficacy Red = predictive of clinical resistance
Sunitinib and regorafenib have complementary activity against imatinib-resistant GIST cell lines *IC50s: Green = predictive of clinical efficacy Red = predictive of clinical resistance
Progression of KIT Exon 13 imatinib-resistant subcloneon regorafenib KIT exon 13 (V654A). Radiographic and metabolic progression on regorafenib Baseline C12D21 Resection biopsy exon 11 + exon 13 (V654A)
Response of KITExon 17 imatinib-resistant subclone on regorafenib KIT exon 17 (D820Y). Radiographic and metabolic response on regorafenib Baseline Pre-regorafenib exon 11 + exon 17 (D820Y) C4D21
Sunitinib and regorafenib have complementary activity against IM-resistant KIT mutations
Targeting TKI-resistance heterogeneity in GIST ATP-binding pocket SUNITINIB Activation Loop REGORAFENIB Cycling sunitinib and regorafenib might suppress a broader spectrum of imatinib-resistant GIST clones and achieve prolonged long-term disease control
Time-frame for restoration of kinase signaling and proliferation after TKI withdrawal TKI withdrawal • Phosphorylation of KIT • Phosphorylation of downstream • signal intermediates (AKT and ERK) • Increase of Cyclin A expression • Increase of Ki-67 expression • Mitotic activity
Sunitinibwashout: reactivation of KIT, downstream pathways, and cell cycle GIST430/654 exon 11 + exon 13 Sunitinib treatment SU 500nM Days of drug withdrawal DAY 3 DAY 1 DAY 0 DAY 7 pKIT Y703 pAKT S473 pRB S795 Cyclin A Actin
Sunitinibwashout: reactivation of KIT, downstream pathways, and cell cycle GIST430/654 exon 11 + exon 13 Sunitinib treatment SU 500nM Days of drug withdrawal DAY 3 DAY 1 DAY 0 DAY 7 pKIT Y703 pAKT S473 pRB S795 Cyclin A Actin
Sunitinibwashout: reactivation of KIT, downstream pathways, and cell cycle GIST430/654 exon 11 + exon 13 Sunitinib treatment SU 500nM Days of drug withdrawal DAY 3 DAY 1 DAY 0 DAY 7 pKIT Y703 pAKT S473 pRB S795 Cyclin A Actin
Sunitinib washout: reactivation of proliferation GIST430/654 exon 11 + exon 13 Sunitinib treatment Untreated SU 100nM SU 500nM Day 0 KI-67 expression Day 1 Day 3 Day 7
Sunitinib washout: reactivation of proliferation GIST430/654 exon 11 + exon 13 Sunitinib treatment Untreated SU 100nM SU 500nM Day 0 KI-67 expression Day 1 Day 3 Day 7
Regorafenib washout: reactivation of KIT, downstream pathways, and cell cycle GIST48/820 exon 11 + exon 17 Regorafenib treatment REGO 500nM Days of drug withdrawal DAY 3 DAY 1 DAY 0 DAY 7 pKIT Y703 pAKT S473 pRB S795 Cyclin A Actin
Regorafenib washout: reactivation of KIT, downstream pathways, and cell cycle GIST48/820 exon 11 + exon 17 Regorafenib treatment REGO 500nM Days of drug withdrawal DAY 3 DAY 1 DAY 0 DAY 7 pKIT Y703 pAKT S473 pRB S795 Cyclin A Actin
Regorafenib washout: reactivation of KIT, downstream pathways, and cell cycle GIST48/820 exon 11 + exon 17 Regorafenib treatment REGO 500nM Days of drug withdrawal DAY 3 DAY 1 DAY 0 DAY 7 pKIT Y703 pAKT S473 pRB S795 Cyclin A Actin
Regorafenib washout: reactivation of proliferation GIST48/820 exon 11 + exon 17 Regorafenib treatment Untreated REGO 100nM REGO 500nM Day 0 KI-67 expression Day 1 Day 3 Day 7
Regorafenib washout: reactivation of proliferation GIST48/820 exon 11 + exon 17 Regorafenib treatment Untreated REGO 100nM REGO 500nM Day 0 KI-67 expression Day 1 Day 3 Day 7
Once a KIT inhibitor is withdrawn: • Phosphorylation of KIT • Phosphorylation of downstream • signal intermediates (AKT and ERK) • Increase of Cyclin A expression • Increase of Ki-67 expression • Mitotic activity 2 days 4 days 7 days
Recovery of mitotic activity in GIST patients responding to TKI therapy after withdrawal of the KIT inhibitor
Rapid alternation regimen 3 days SU 4 days REGO 4 days REGO 3 days SU • Rapid alternation regimen might minimize toxic effects. • Alternation of complementary drugs increases the spectrum of effective inhibition of IM-resistant clones.
Conclusions Sunitinib and regorafenib have complementary activity against secondary KIT mutations. After withdrawal of an effective KIT inhibitor, target re-activation occurs in 1 to 3 days. Proliferation markers are re-activated between 3 to 7 days, and mitotic activation is observed in vitro and in clinical correlates between 4 to 7 days. These observations define a rational schedule for alternation of sunitinib and regorafenib in a heterogeneous GIST population that will be shortly tested in a Phase Ib clinical trial.
Co-authors / Acknowledgments Brigham and Women’s Hospital Ludwig Center at Dana-Farber Cancer Institute Jonathan Fletcher Lab Jonathan A. Fletcher Grant Eilers Albert Ha AdriánMariño-Enríquez Anna Quattrone Gloria Ravegnini Inga-Marie Schaefer Derrick Tao Yue-Xiang Wang Mei-Jun Zhu Pathology Department Christopher D.M. Fletcher Leona A. Doyle Jason Hornick Division of Surgical Oncology Chandrajit P. Raut George D. Demetri James E. Butrynski David R. D’Adamo Suzanne George Jeffrey A. Morgan Andrew J. Wagner Lerner Research Institute and Cleveland Clinic Anu Gupta Brian P. Rubin West German Cancer Center Sebastian Bauer Valld’Hebron University Hospital Joan CarlesGalcerán ASCO Young Investigator Award Spanish Society of Medical Oncology Translational Award Faculty from the 2013 Flims Workshop GIST Cancer Research Fund, The LifeRaft Group Virginia and Daniel K. Ludwig Trust for Cancer Research