Download
1 / 78
800 likes | 868 Vues
Explore the role of DAX-1 gene in Dosage Sensitive Sex Reversal and Adrenal hypoplasia congenita on the X chromosome in human females. Learn about follicle formation, estrogen actions, ovarian cycles, Turner’s Syndrome variants, PCOD diagnosis, and treatment options.

E N D
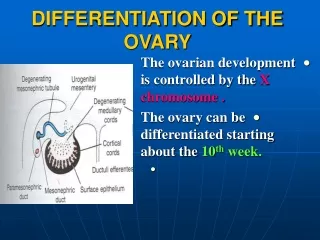
THE OVARY DETERMINATION: DAX-1 geneon the short arm of X chromosomeXp21 DAX-1= Dosage Sensitive Sex Reversal / Adrenal hypoplasia congenita on the x chromosome
In human females, all primordial follicles are formed in the fetus between 6 and 9 months' gestation. During this period, there occurs a marked loss of oocytes due to apoptosis. The number of primordial follicles decreases progressively as a consequence of recruitment, until very few if any are present after the menopause at ~50 years of age. (Baker TG: Radiosensitivity of mammalian oocytes with particular reference to the human female. Am J Obstet Gynecol 110:746, 1971. Reproduced with permission from Mosby, Inc.)
The early differentiation of the granulosa cells during preantral folliculogenesis involves the expression of FSH receptors. Animal studies support the concept that this process involves an activin autocrine/paracrine mechanism. (Erickson GF: Dissociation of Endocrine and Gametogenic Ovarian Function. In Lobo, R. (ed.): Perimenopause. Serono Symposia, Springer-Verlaag, 1997. Reproduced with permission from Springer-Verlag, New York.)
CONTROL OF OVARIAN FUNCTION : THE 2 CELL – 2 GONADOTROPIN HYPOTHESIS
Diagram showing the "Two Gonadotropin-Two Cell Concept" of follicle estrogen production. (Erickson, GF: Normal ovarian function. Clin Obstet Gynecol 21:31, 1978. Reproduced with permission from Lippincott-Raven Publishers.)
ENDOMETRIAL CYCLE
ASSESSMENT OF OVARIAN FUNCTION • ESTRADIOL • PROGESTERONE • FSH • LH • LHRH TEST • SHBG • PROLACTIN • TESTOSTERONE (FREE) • DHEA-S • BASAL BODY TEMPERATURE • CERVICAL MUCUS • ENDOMETRIAL BIOPSY • ULTRASOUND EXAMINATION • LAPAROSCOPY
ASSESSMENT OF OVARIANFUNCTION ESTRADIOL, FSH, LH, PROLACTIN E2 FSH LH E2 FSH LH PROLACTIN E2 FSH LH LHRH test HIPERPROLACTINEMIA - + HYPOTHALAMUS PITUITARY HYPOGONADOTROPIC HYPOGONADISM HYPERGONADOTROPIC HYPOGONADISM
MENSTRUAL PROBLEMS • PRIMARY AMENORRHEA • SECONDARY AMENORRHEA • OLIGOMENORRHEA • DYSMENORRHEA
TURNER’S SYNDROME AND ITS VARIANTS PREVALENCE:1/5000 FEMALE NEWBORN 99 % of fetuses 45,X do not survive over 20 week of gestation 15 % of spontaneous abortions of the first trimester CLINICal data: Short stature <145 cm in forma 45,X, or less than -2 Sd from the normal malformations: 200 malformatii somativ and visceral Primary amenorrhea
TURNER’S SYNDROME AND ITS VARIANTS Genetics: 45,X, 45, X/46,XX, 46, X Xqi, 46, X X “ring chromosome” Diagnostics: • absence of Barr body • low estradiol • FSH/LH increased ( over 40 mIU/mL) • ultrasound and other diagnostic methods for malformation
TURNER’S SYNDROME AND ITS VARIANTS TREATAMENT objectives: Growth • hrGH: 0,05 mg /kg bw/day with a growth increase of 8-10 cm than without treatment • ± oxandrolone: 0,0625 mg/kg/day Development of secondary sexual characteristics and menses: • conjugated estrogens 0,3 mg /zi 21 day , or EE2 =5 microg /day 21 days • progesterone is given later Pregnancy: surogate mothers
Polycystic ovary disease (syndrome) PCOD or PCOS is a complex entity with a pathogenicy not fully understood which can affec 5-10 % of women in their reproductive age. Is the most frequent cause of endocrine infertility. The disease is characterized by the following criteria: • Clinical: chronic anovulation, hirsutism (excess of facial and body hair sometimes with male-like distribution), menstrual abnormalities, obesity • Biological (hormonal): increased plama androgens, LH/FSH ratio increased over 2 • Histological and ultrasound: the presence of at least 10 cystic follicle on every ovary . The biological picture may be seen without polycystic ovary on ultrasound or polycystic ovary in ultrasound examination with apparently normal ovarian function.
Polycystic ovary disease (syndrome) ethiopathogenity • Initial neuro endocrine abnormality with increased amplitude and frequency of pulses of LH-RH due to lost of inhibitory control physiologically produced by dopamine and opioids with permanently increased LH level. Permanently increased LH levels are responsible for increased androgen secretion in the theca interna and chronic anovulation • Initial increased secretion of ovarian androgens may be the result of a genetic increased activity of 17 α hydroxilase (p450 C17α). In some cases an increased production of adrenal androgens due to late onset of CAH with 21 hydroxilase deficiency or 11 hydroxilase deficicency • Functional deficiency in androgen aromatisation. In the concept of “two cell-two gonadotropins” control of ovarian function the PCOD may rezult from a desechilibrium between factors that facilitate androgen secretion (LH and insulin) and those which control aromatisation, selection of dominant follicle, proliferation of theca granulosa (FSH, inhibin hypersecretion)
Polycystic ovary disease (syndrome) ethiopathogenity • Primary insulin resistance or insulin resistance secondary to obesity. Insulin is known to normally stimulate androgen secretion in the ca interna. Increased insulin level produces theca interna stimulation of androgens, decreases Sex Hormone Binding Globulin (SHBG) therefore increasing testosterone biodisponibility to tissues. In the adipose tissue it is and increased aromatisation of peripheral androgens with increase extraovarian production of estradiol that in turn decreases FSH and rezults in chronic anovulation.